



I. INTRODUCTION
Skin lesions by surgeries or trauma results in the formation of scars. Facial scars have psychological effects, as they are impossible to hide, the main clinical objective of the treatment is being to repair the skin and minimize the scar. Surgeons expend time to improve the aesthetic appearance of the skin during repair of trauma or surgery .
However, most techniques used for scar reductions reduce, instead of eliminating, the muscular system acts on the scar. The underlying musculature produces a hard tension over the wound, therefore, these muscles must be paralyzed using botulinum toxin A (BTA). BTA blocks the acetylcholine release at the neuromuscular junction, producing paralysis .
BTA is useful to treat of various medical conditions, and increasingly used in aesthetic medicine. The action of the drug includes diminish wound tension, collagen production, and fibroblasts growth. BTA also works inhibiting the presynaptic release of acetylcholine, as it acts at the neuromuscular junction .
The administration of BTA causes muscle paralysis which may last from two to six months. It has been used for medical purposes since the 1980s and the use of BTA in the treatment of pathological scars was first reported in 2000. To date, its mechanism is still not clearly understood. In recent years, an increasing number of doctors have preferred intralesional BTA for the prevention and treatment of hypertrophic scars and keloids combined or not with other therapy .
The mechanism of wound healing is sophisticated and simultaneous process occurs in three stages: inflammation, granulation tissue formation, and matrix formation. If there are changes in these healing stages, it may result in the formation of pathological scars .
The most important factor that defines the appearance of a scar is the force tension over the wound edges during the healing process. The injection of BTA reduces the perpendicular tension on the wound edges and muscular force over the skin, inhibiting the formation of hypertrophic scars and keloids. BTA allows almost complete inhibition of dynamic muscle tension in the edge of the wound during the healing process[2,3,5,6,7]. The present study aimed to demonstrate the use of botulinum toxin as a possible treatment for reducing facial scarring.
II. METHODS
This is a retrospective study involving patients treated at clinic who were treated with BTA the management of facial wounds. Qualitative analyses of the evolution of the treated patients were performed. Study approved by the Research Ethics Committee of the Veiga de Almeida University under protocol number 29151320.0.0000.5291.
Clinical Case 1
30-year-old female, had an accident riding a bicycle. She injured her forehead and was treated in the emergency room. On the following day, she went to the clinic concerned with the aesthetic effect of the injury.
BTA was applied to the entire forehead and perilesional area (4ui per puncture). The treatment was repeated after three months.
One year later, there was minimal scarring in the area, and at the last follow-up, an unapparent scar.


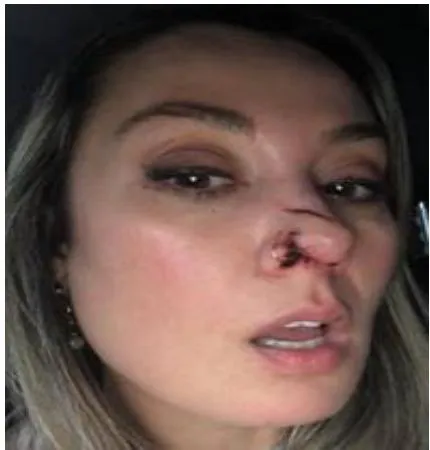
Clinical Case 2
30-year-old female, was attacked by a dog that bit her nose. The patient was seen at the clinic 48 hours after the attack. Botulinum toxin A was applied to all nasal musculature (4ui per puncture in this area). The treatment was repeated after 3 months.
One year later, there was minimal scarring in the area.

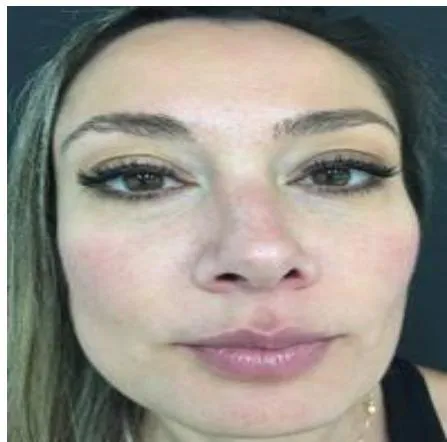
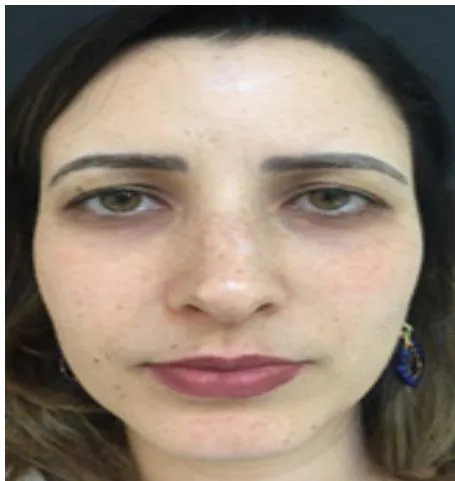
Clinical Case 3
33-year-old female, fell from the stairs and hit a glass door. She came to the Clinic 3 weeks after the accident. At that time she presented scars on the left frontal region and upper left eyelid, as well as scar retraction with enlargement of the scar near the glabellar region. The patient had some muscle movement in the affected area.
Botulinum toxin A was applied to the affected area and to the scar edges (40ui total of the application), requiring retouching in the regions that showed relief and, also, slight scar movement.



III. DISCUSSION
Scars on the face can affect social well-being through a negative image, sometimes inducing psychological disturb. Its possible minimize the scars facilitating healing applying scar care medicine, occlusive or semi-occlusive dressing, high quality suture material and good closure, and avoiding sun exposure[^8].
But, the most important action is reducing the tension on wound edges by applying BTA locally, it may be prevent formation of hypertrophic scars or keloids.
Clinical cases here presented are examples of our experience in recent years using the neuromuscular blockade technique with BTA in facial wounds, which prevents the dynamic movement of the muscles involved, resulting in safe healing and practically invisible scars. Treatment with BTA was proposed for the treatment of hypertrophic scars and keloids in 2014 and .
We have used this technique to treat scars since 2011 (the first case mentioned in this study). Movement produces tension on the edge of the wound, which can be avoid injecting BTA in the region, thus reducing muscle contraction, skin tension, microtrauma, and inflammatory process[^11].
BTA reduce the expression of transforming growth factor-beta, which is the main regulator of the formation of hypertrophic scarring[^3].
Kim YS et al performed a split-scar, double-blind, randomized, controlled study on 15 patients with early post-thyroidectomy scars. After six months they found a significant improvement in of the scar, comparing the BTA area to the saline area[12].
The study of Shaarawy E. et al shows BTA more effective in reducing pruritus and keloid-related pain than intralesional corticosteroids where used to preventing hypertrophic scar .
Moreover, the 3D profilometry used to objectively assess keloids treated with BTA showed a lack of results in some surgical cases. Some clinical studies did not support variations in TGF-beta or fibroblasts after the treatment of scars with BTA. Thus, there are conflicting results from points of view available, and further studies are needed to assess the specific role of BTA in the healing phisiology .
BTA acts during two to six performing temporary chemodenervation by acting on the presynaptic neuron, blocking the release of acetylcholine, leading to functional denervation of the striated muscle .
Regarding of the functional effects of the BTA scar formation maybe takes few months, and our observations of final results depended on the end of the histopathological healing process.
Predictably, the effects of BTA on the maturation of the scar may take more than one month to be visible. Our evaluation, satisfaction and measurement data, demonstrate that the injection of Botulinum Toxin A has a positive effect on scars.
Ziade et al validated scar assessment scales evaluate the healing (texture, size, and color) results of complex wounds, but not to be used in simple facial wounds . Injection of BTA improved significantly the discoloration of the scar. Skin lesions invoke an inflammatory response influencing cellular mediators acting over melanocytes and melanogenesis in several ways. The release of nitric oxide, histamine, p53, and transforming growth factor b1 (TGF-b1) by the inflammatory process induces melanogenesis .
Post-inflammatory hyperpigmentation is still unclear, it is believed that activation of melanocytes is involved through oxidative species and inflammatory mediators by skin wounded[^18].
Since the damage to the skin is caused by repeated microtrauma due to the movement of the injured tissue (skin traction), it provokes a prolonged release of peptide related to the calcitonin gene and substance P, in addition to the cleavage of the SNAP25 protein, by injection of . With these factors together we can observe that the stress-relieving properties of BTA added to its inhibiting effects on inflammation support the use of the drug in preventing scarring.
IV. CONCLUSION
Botulinum toxin A is efficient for the treatment and reduction of facial scars resulting from trauma or surgical interventions. This study shows a reduction in the size and pigmentation of scars in patients who were treated with a perilesional injection of BTA, which may be a choice method for avoiding or treat hypertrophic scars and keloids in areas of muscle tension. This study demonstrates good clinical effects of BTA in the treatment and prevention of hypertrophic scars and keloids.



