## I. BACKGROUND
Metroplasty, first illustrated in 1907 by Strassman, is a reconstructive surgery used to repair congenital anomalies of the uterus including septate, bicornuate and didelphys uterus. This surgery involves removal of the abnormal tissue that separates the uterine cornua, and then creating a normal shaped uterus by suturing in multiple layers.
septate uterus, i.e., 60% Although most women with Mullerian anomalies can conceive without difficulty, obstetric complications and adverse pregnancy outcomes have been more commonly reported in anomalous uteri. They are associated with a high rate of recurrent spontaneous abortions, preterm labour, cervical incompetence, malpresentations, foetal growth restriction, high risk of uterine rupture, retained placenta and post-partum haemorrhage. Risk of pregnancy wastage differ with the type of uterine anomaly—maximally in bicornuate and septate uterus, i.e., $60\%$, $55\%$ in uni-cornuate and didelphys uteri and $35\%$ in arcuate uterus. $^{2}$ Uterine anomalies are seen in approximately $12.6\%$ (1.8-37.6%) of patients with recurrent pregnancy loss as compared with $4.3\%$ (2.7-16.7%) of the general population. $^{2}$ Often, they are seen accompanying various renal anomalies. According to Thompson and Lynn, $^{3}$ $40\%$ of females with congenital absence of the kidney are found to have associated genital anomalies.
Surgical interventions are indicated when there is obstruction causing associated pelvic pain and endometriosis and for women with poor obstetric outcomes. Before metroplasty, extra-uterine causes need to be ruled out. The goals of metroplasty are restoration of pelvic anatomy, preservation of fertility, and treatment of pelvic pain and endometriosis.
We hereby discuss 5 cases of congenitally anomalous uteri, in whom we performed metroplasty.
## II. CASE DESCRIPTION
The procedure was initiated by a transverse incision in the lower abdomen through which the abdomen was opened and uterus was visualised. To minimise the blood loss, injection vasopressin was injected into the myometrium or temporary bilateral uterine artery ligation was done using a constricting Foley's catheter. In cases of bicornuate and didelphys uteri, both the cornua are deeply incised on the median side in their long axis to expose both the uterine cavities. Care was taken to avoid injury to the fallopian tubes. The cut edges of the myometrium were then approximated and sutured vertically anteriorly and posteriorly with Vicryl 2-0 in continuous manner in three layers in order to create a single uterine cavity.
Case 1: OHVIRA/Herlyn-Werner-Wunderlich Syndrome: Uterine didelphys + Hematometra/ Hematocolpos + Absent Right Kidney
A 28-year-old female, married for 10 years, presented with Primary infertility. Pelvic examination showed unicollis and presence of bogginess in the right lateral fornix.
USG showed absence of right kidney and two separate uterine cavities and cervices- s/o Uterine didelphys. ESHRE Classification U3BC2, with approximately equally sized right and left horns. A collection of $\sim 5\mathrm{cc}$ was seen in right cervical canal and upper third of vagina s/o Hematometra + Hematocolpos.
The two uterine horns were united by metroplasty, and follow-up USG showed a single uterine cavity with resolution of hematometra and hematocolpos. (Fig. 1)
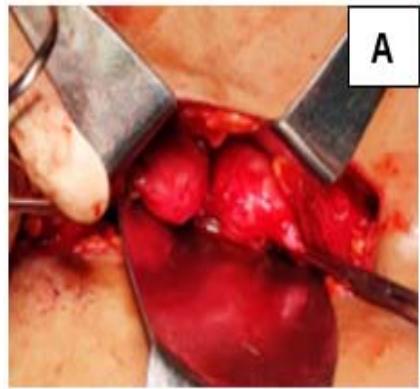
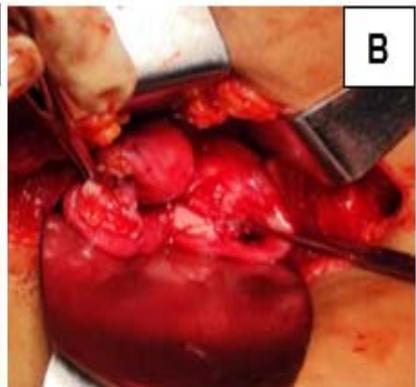
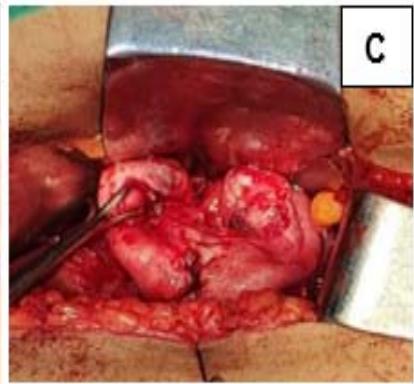 Figure 1: A: Uterine didelphys. B: Cavity opened. C: Edges of cavity approximated and sutured.
### Case 2: Bicornuate Uterus
A 33-year-old female, married for 9 years, with previous 2 spontaneous abortions at 4-5 months of gestation, presented with secondary infertility. USG and
HSG revealed bicornuate uterus with approximately equal sized right and left horns. Metroplasty was performed and follow-up USG showed a single uterine cavity. (Fig. 2)

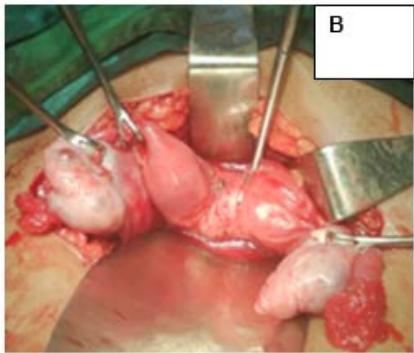
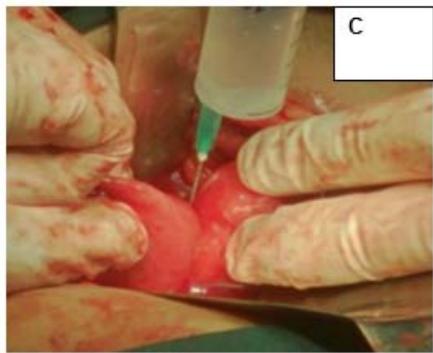
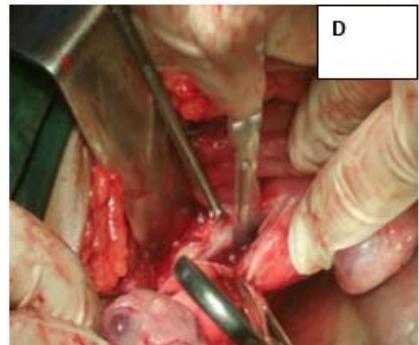
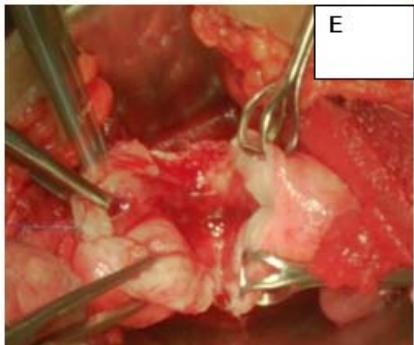
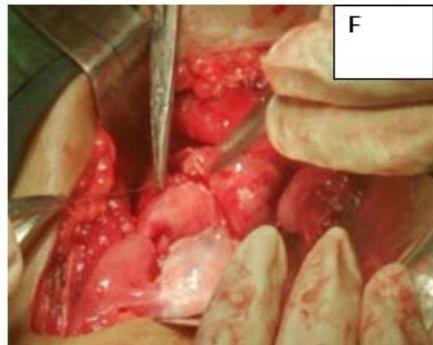 Figure 2: A: HSG s/o Bicornuate uterus. B: Bicornuate uterus on laparotomy. C: Vasopressin injected to minimize the blood loss during surgery. D: Transverse incision taken over uterine fundus. E: Uterine cavity opened. F: Edges approximated & sutured vertically
#### Case 3: Bicornuate Uterus
A 35-year-old, female married for 8 years, with a spontaneous abortion at $4^{\text{th}}$ month of gestation, presented with Secondary infertility. USG showed bicornuate uterus with almost equal right and left horns, communicating in the lower third of the uterus, s/o Bicornuate uterus. ESHRE Class: U3a. HSG confirmed the same. Follow up- HSG post metroplasty showed resolution with slight depression in the fundal region. (Fig. 3)
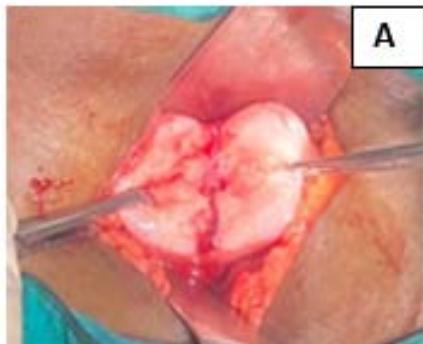

 Figure 3: A: Opening the uterine cavity for metroplasty. B and C: Comparison of pre-op and post-op HSG
#### Case 4: Bicornuate Uterus
A 34-year-old female married for 9 years, with 4 spontaneous abortions at 3-4 months of gestation, presented with secondary infertility. USG showed Bicornuate uterus with almost equal right and left horns, communicating in the lower third of the uterus, s/o Bicornuate uterus, with HSG confirming the diagnosis. Post metroplasty, she had a successful pregnancy till term and underwent LSCS uneventfully. (Fig. 4)
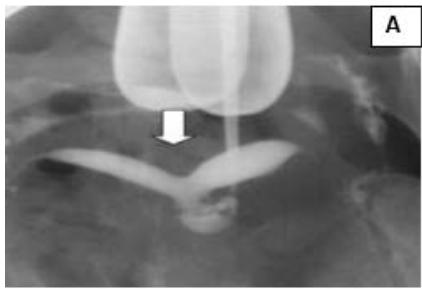

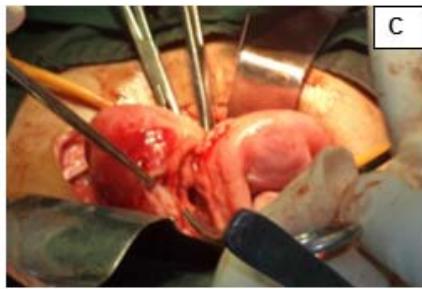
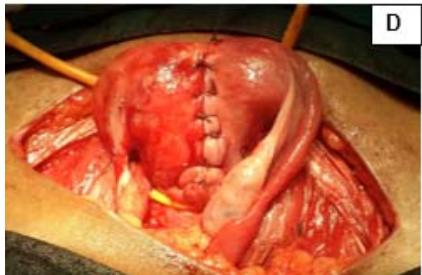
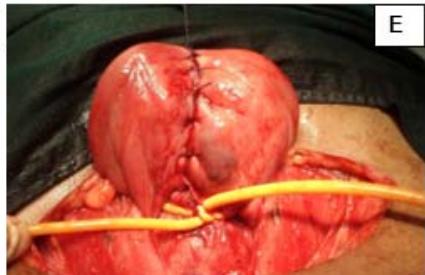
 Figure 4: A: HSG s/o Bicornuate uterus. B: Bicornuate uterus. C: Temporary ligation with Foley and opening uterine cavity. D and E: Anterior and posterior surface after suturing. F: Healed uterus as seen during Caesarean section.
#### Case 5: Uterine didelphys with high vaginal septum
A 29-year-old, female married for 2 years, nulligravida, presented with dyspareunia and primary infertility. Patient was a known case of uterine didelphys with vertical vaginal septum and gives history of being operated for imperforated anus in childhood. Pelvic examination showed complete vertical vaginal septum with two vaginal canal leading to two separate cervices. Both the cervices were short and flushed with vagina and UCL was measured as 3 inches on both sides. USG showed uterine didelphys with vertical vaginal septum. Patient underwent vaginoplasty and metroplasty and post operatively, dilatation with Hegars No. 28 dilators was advised. The patient was able to have normal sexual function. (Fig. 5)





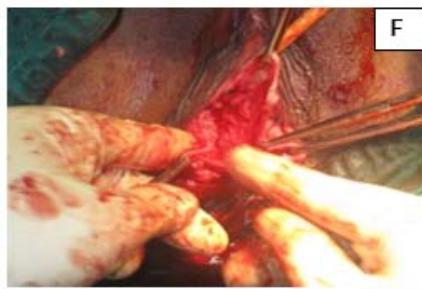

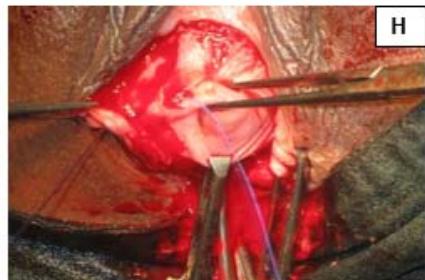
 Figure 5: A: Uterine didelphys. B: Opening cavity during metroplasty. C: Complete vertical septum infiltrated with saline. D: Vaginal canals opening into two separate cervical openings. E: Anterior lip of cervices held with Allis' forceps and vertical incision taken over septum. F: Plane of dissection maintained along the septum. G: Redundant mucosa cut. H: Cut ends sutured with vagina with Vicryl 3-0. I: Vagina with two cervices.
Post procedure, the patients were advised to avoid conception for at least 1 to 2 years and all future pregnancies are to be terminated by Caesarean section to avoid risk of uterine rupture at the relatively weak suture sites during labour.
All women were advised a repeat HSG and USG after 3 months, which in all the cases confirmed the unison of the uteri into a single cavity.
## III. DISCUSSION AND CLINICAL SIGNIFICANCE
Surgery is not a rule for all cases of uterine anomalies. Most women with minor uterine anomalies conceive spontaneously and carry pregnancy till term. However, metroplasty is indicated when there is history of two or more fetal wastages, and when other causes are ruled out.
A review of literature reveals that Strassman metroplasty significantly improves the obstetric outcomes in women with Mullerian anomalies. The rate of fetal wastage prior to metroplasty was found to range from $70 - 88\%$ in various studies, in comparison to live birth rates of $81 - 85\%$ after metroplasty.[5-11]
Prior to abdominal metroplasty, the uterine anomaly needs to be confirmed. Accuracy of hysterosalpingogram alone is only $55\%$ for differentiation of septate uterus from the bicornuate uterus $^{13}$, and hence is confirmed by 3-D USG and MRI. A more suitable modality in settings where facilities are available, hystero-laparoscopy can be performed, wherein septate uterus, when detected can be corrected by hysteroscopic resection in the same setting, with minimal invasion, thus avoiding unnecessary laparotomies. However, the enlarging use of hysteroscopic metroplasty is not wholesome as it may create cervical fragilization, thus necessitating a cervical cerclage in order to prevent $2^{\text{nd}}$ trimester pregnancy loss. The abdominal metroplasty still remains the operation of choice destined to treat cases of bicornuate uterus or uterus didelphys due to high risk of perforation during hysteroscopic correction.
Generating HTML Viewer...
References
12 Cites in Article
B Hoffman (2016). Review of Williams et al. 2016.
G Grimbizis,M Camus,B Tarlatzis,J Bontis,P Devroey (2001). Clinical implications of uterine malformations and hysteroscopic treatment results.
Dennis Thompson,Hugh Lynn (1966). GENITAL ANOMALIES ASSOCIATED WITH SOLITARY KIDNEY.
Beth Rackow,Aydin Arici (2007). Reproductive performance of women with müllerian anomalies.
Hayden Homer,Anthony (2018). Modern management of recurrent miscarriage.
E Strassman (1966). Fertility and Unification of Double Uterus.
Z Papp,G Mezei,M Gávai,P Hupuczi,J Urbancsek (2006). Reproductive performance after transabdominal metroplasty: a review of 157 consecutive cases.
R Tomasz,M Marta,B Aleksandra (2009). Clinical effectiveness of Strassman operation in the treatment of bicornuate uterus.
F Valle,R (1996). Hysteroscopic treatment of partial and complete uterine septum.
D Lolis,M Paschopoulos,G Makrydimas (2005). Reproductive outcome after Strassman metroplasty in women with a bicornuate uterus.
R Tomasz,M Marta,B Aleksandra (2009). Clinical effectiveness of Strassman operation in the treatment of bicornuate uterus.
Perrine Juillion What is the difference between bicornuate and didelphys uterus? Available at.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Adithi Jayaprakash. 2026. \u201cUniting the Uteri: A Case Series\u201d. Global Journal of Medical Research - E: Gynecology & Obstetrics GJMR-E Volume 23 (GJMR Volume 23 Issue E1): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































