## I. INTRODUCTION
Scoliosis is a three-dimensional spinal curve with side-to-side curve(s) and spinal rotation. It affects $2 - 3\%$ of the world's population. $^{1}$ Of Earth's approximately 8 billion people, 160 - 240 million people suffer from scoliosis. Effective antibiotics for tuberculosis and vaccines for polio have made adolescent idiopathic scoliosis (AIS) nearly $90\%$ of all $\text{scoliosis}^{2}$ Females are more likely than males to acquire the condition, the ratio changing from 1.4:1 in curves of 10-20 degrees to 7.2:1 in curves above 40 degrees. $^{2}$ Although asymmetric sports such as tennis and baseball have no bearing on scoliosis, dancing significantly raises the risk. $^{3}$ It is uncertain whether this is due to ligamentous and bone changes or to the greater flexibility of dancers, enabling asymmetric forces to curve the spine more readily.
When a curve's Cobb angle exceeds 25 degrees, braces are often implemented to deter progression, since this is the level at which most studies report the highest rates of progression.4-7 However, several other systems make their own determinations: The Rigo-Cheneau classification stipulates its own guidelines for implementation, and designs and crafts braces in ways that may depart somewhat from the 25-degree demarcation.8 It coordinates brace design with fabrication, using its own principles of correction, and thus has control over the relationship between when to prescribe and what is furnished. The soft Spine-Cor brace has its own system as well, with its own parameters of internal consistency.9
Generally, braces are not expected to diminish curvature but rather reduce curve progression. $^{10}$ Nevertheless, the Spine-Cor and Lyons braces have been reported to have corrective capacities. $^{11,12}$ When the goals of bracing were polled among authorities in the field, aesthetics, quality of life, disability, back pain and psychological well-being were found to be the most important goals in that order. $^{13}$ These goals are promoted naturally through curve correction as well. The same group judged the evidence in favor of bracing to be stronger than the evidence for any other conservative modality, with scoliosis-specific exercises second. $^{14}$ Nevertheless, discomfort, embarrassment at school, lowered self-esteem, body image $^{14}$ and consequent issues of compliance are relevant, and questions have been raised about whether core stabilization, scoliosis-specific exercises, and even the use of a second orthotic or insoles improve braces' efficacy. $^{13,15}$
Other conservative methods, such as the Schroth, and chiropractic systems, such as Pettibone and Clear, have mixed reports regarding efficacy, and physical therapeutic exercise programs are also currently being tested.[16-19] Greater clarity on ancillary treatments with braces is desirable, especially concerning the underlying principles that can guide therapeutic decisions.
Typically, surgical intervention is considered only when curves exceed 45 degrees. Surgery has rightfully dominated the field of scoliosis since it has been the most reliable and effective remediation for many years. The natural history of AIS suggests 0.4 to 2.2 degrees of annual progression, depending upon age, Risser number and curve type, although teenagers' spines are capable of much greater change.[4-6] When visiting their surgeons, young patients have an X-ray taken, and they and their families often are told of the 45-degree threshold for surgery. With or without braces, parents and their children with AIS are relegated to the passive role of "watchful waiting" unless and until curves reach 45 degrees.
Although genetic, anatomical and neuroanatomical correlates of AIS have been discovered[20-23] promising physiotherapeutic work to effectively stabilize and reverse scoliosis awaits high-quality studies that confirm it.[24] A reliable, innocuous method would be particularly valuable since, unlike major surgery, it could be instituted in patients with much smaller curves, when treatment would commence earlier and likely would not be as disruptive nor last as long.
Previous work suggests electrophysiological and hormonal muscular asymmetries are at work in AIS,[25,26] supporting the possibility that muscular imbalance may be a relevant factor in its pathogenesis. We tested this hypothesis by utilizing botulinum toxin type A, incobotulinum, a medication that temporarily weakens muscles, on the concave side of lumbar curves, and an asymmetrical yoga pose, the side plank, to strengthen the convex side. Incobotulinum has few other effects after intramuscular injection.
The hypothesis that muscular imbalance is important in AIS is also supported by a study finding that the Schroth method, a muscle-oriented treatment, significantly improved curves.[19] Further, this single yoga pose, the side plank, performed with the convex side of lumbar curves held inferiorly, was found to be helpful in lumbar AIS in multiple studies.[27-29] A randomized, controlled repeat of this method found it ineffective,[30] but close reading of that study reveals that unfortunately, the randomization of the intervention group was such that not a single patient with a lumbar curve was included in it.[31] In the current study, we used the side plank to strengthen the weaker (convex) side and added incobotulinum injections of the contralateral (concave) paraspinal, quadratus lumborum and psoas muscles to temporarily weaken the stronger side. Bracing of patients was not permitted during the test period to avoid a confounding factor. Testing the validity of the muscular imbalance hypothesis, the primary and secondary objectives of this study were to assess the benefits and the harms[32] of combining incobotulinum injections with yoga to reverse lumbar and thoracolumbar AIS.<sup>28-30</sup>
The current study has been approved by the Chesapeake IRB (now Advarra) and the FDA, since this use of botulinum toxin is virtually new in the United States. One other institution is studying it in a similar context.[33] The current study was made public on Clinical Trials.org NCT04922983 on 17 July 2021 and was accessed on that day. Recruitment began 17 July 2021.
## II. METHODS
This is a randomized, controlled study, with two non-botulinum groups: Group 1 received a placebo yoga pose only, while Group 2 received the intervention yoga pose and preservative-free normal saline (placebo) injections. The full intervention group, Group 3 received both the interventional yoga pose and botulinum injections.
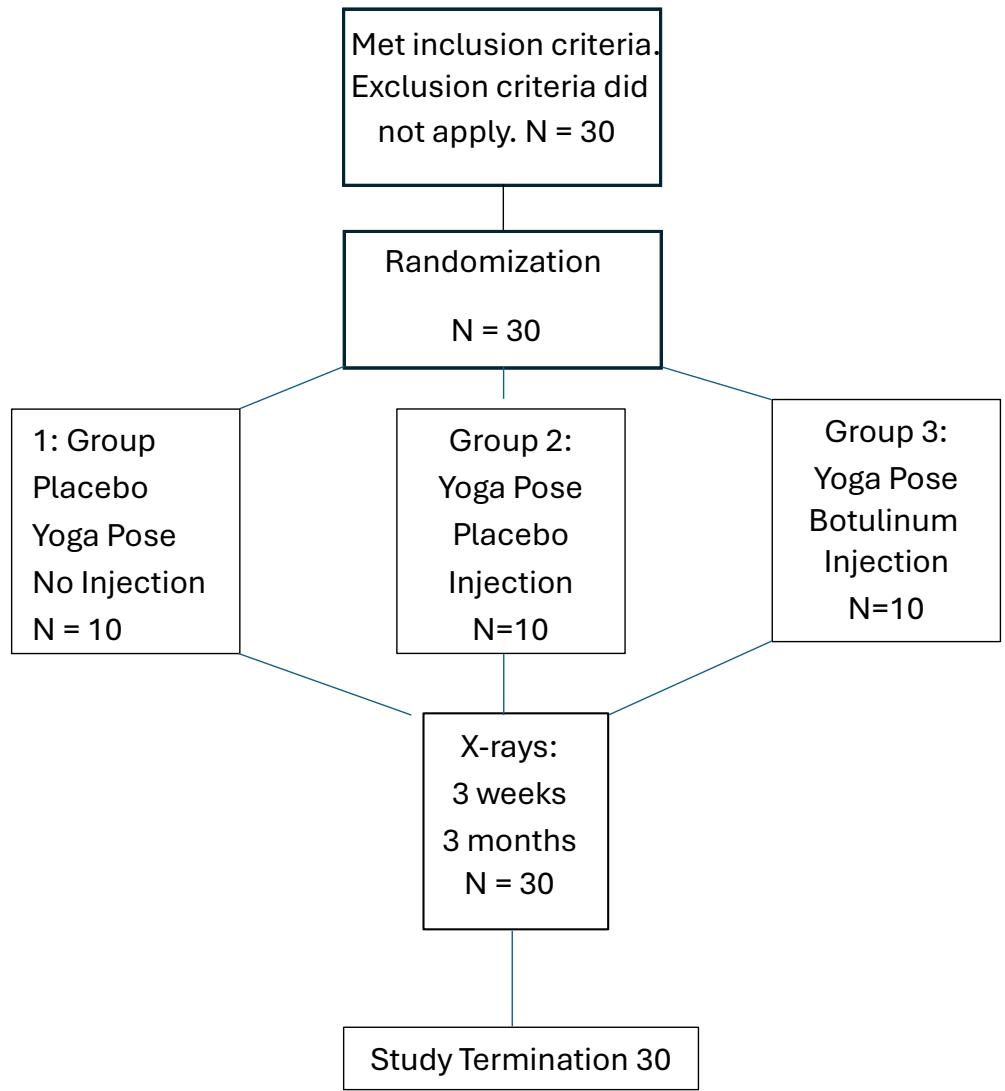
Figure 1: Flow Chart
### a) Eligibility
## i. Inclusion Criteria
- Age 12-20 years.
- Lumbar or thoracolumbar curve of $25^{\circ} - 45^{\circ}$
- Willingness to perform one yoga pose for as long as possible three times daily for three months.
- Parental or guardian agreement.
## ii. Exclusion Criteria
- Neuromuscular or musculoskeletal disease, e.g., cerebral palsy, Guillain-Barre syndrome, Marfan's syndrome.
- Current use of brace.
- Previous spinal surgery.
- Previous exposure to botulinum toxin type A.
- Positive pregnancy test.
## iii. Particulars of the Study
The study was conducted in private offices in Manhattan, New York, USA.
The study accepted non-pregnant applicants who had $25^{\circ} - 45^{\circ}$ lumbar or thoracolumbar curves on Cobb X-rays completed less than 6 months before their visits. Group 1 patients were given a regular yoga pose, the plank, that consists of a symmetrical two-handed suspension of the upper body with extended elbows and lower body suspended on dorsiflexed feet. Group 2 patients were given the side-plate (Vasisthasana) in which the body is supported by one extended arm with the torso's coronal plane perpendicular to the floor and the lower body weight supported by the posterolateral foot of the convex side of the curve, and placebo injection of 0.33 cc normal saline injected into each muscle: the lumbar paraspinals opposite the apex of the curve, the quadratus lumborum opposite L3, and the psoas with needle entry approximately 7 cm. lateral to the L4 spinous process. Group 3 patients were given the side plank and injections of 33 IU incobotulinum into these same muscles. All injections were given on the curves' concave sides. Paraspinal and quadratus lumborum injections were performed with 1.5 inch inject needles; the psoas injection was performed with a 7 inch inojct needle; all injections were conducted under EMG guidance. Instructions to both placebo and interventional participants were that poses were to be performed three times daily for as long as possible each time. Patients' vital signs and weight were tested before the injections and again (except for weight) $15\mathrm{min}$ after the injections. Patients repeated their scoliosis X-rays at 3 weeks and 3 months. EOS technology was used whenever possible to minimize exposure to radiation. Checks on participants' compliance with the threetimes-daily full plank or side plank regimen were made by telephone and email.
Power calculations based on previous papers[23-25] yielded 10 subjects in the control group and ten subjects in the study group, where alpha = 0.05 and (1 - beta) = 80%, (10 subjects per group). Statistical measures included regression analyses, both crude and adjusted for age, weight, Risser score, and sex. Randomization was conducted through random.org as patients qualified for the study presented in the office. There was no blocking.
Each patient or the parents of patients under 18 read and signed the Informed Consent Form. A medical assistant enrolled the patients; the office manager generated the randomized treatment group. The medical assistant prepared the syringe with preservative-free normal saline or lyophilized incobotulinum plus 1 cc of preservative-free normal saline, both colorless liquids. The participants, care providers and radiologists performing the initial and subsequent scoliosis X-rays and measuring Cobb angles were all blinded regarding group assignment. Apart from Group 1, which performed the two-handed 'placebo' yoga pose, and which of necessity was different in appearance from the intervention yoga pose, and the fact that this group had no injection, all procedures were indistinguishable to participants, care givers and radiologists. Mixed effects regression analyses were used to test the hypotheses, since differences between three groups was sought.
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional Review Board CIRBI of Advarra on December 2, 2020.
It was registered at ClinicalTrials.org at NCT04922983 on 17 July 2021.
## III. RESULTS
Groups 1 and 2 made up control groups of 10 patients each, with 3 males in each group. Group 3 had 10 patients with one male. (See figure 1.) Mean age of controls and intervention patients: Group 1: 16.2 (S.D. 2.5); Group 2: 16.8 (2.8); Group 3: 15.8 (2.0). Mean weight of controls and intervention groups: Group 1: 119.3 lb. (10.7); Group 2: 117.5 lb. (20.2); Group 3: 126.7 lb. (13.0). Risser numbers: Group 1: 3.96 (.9) Group 2: 3.6 (1.4) Group 3: 3.7 (.7)
Table 1: Demographics Group Age Male Wt Side Size Type R# FHx Group 1 16.22 3 119.33 6 Rt 29.8 4S,2L,4TL 3.96 50% SD 2.49 10.7 6.89 0.93 Group 2 16.8 3 117.5 3 Rt 38.1 5S,2L,3TL 3.6 60% SD 2.80 20.17 7.97 1.4 Group 3 15.8 1 120.1 2 Rt 33 3S,3L,4TL 3.8 50% SD 2.00 20.17 6.31 0.73 Mean 15.1 119.0 3.7 Rt 33.63 2.6S,4.3 L,4TL 3.7 53%
<table><tr><td>Group</td><td>Age</td><td>Male</td><td>Wt</td><td>Side</td><td>Size</td><td>Type</td><td>R#</td><td>FHx</td></tr><tr><td>Group 1</td><td>16.22</td><td>3</td><td>119.33</td><td>6 Rt</td><td>29.8</td><td>4S,2L,4TL</td><td>3.96</td><td>50%</td></tr><tr><td>SD</td><td>2.49</td><td></td><td>10.7</td><td></td><td>6.89</td><td></td><td>0.93</td><td></td></tr><tr><td>Group 2</td><td>16.8</td><td>3</td><td>117.5</td><td>3 Rt</td><td>38.1</td><td>5S,2L,3TL</td><td>3.6</td><td>60%</td></tr><tr><td>SD</td><td>2.80</td><td></td><td>20.17</td><td></td><td>7.97</td><td></td><td>1.4</td><td></td></tr><tr><td>Group 3</td><td>15.8</td><td>1</td><td>120.1</td><td>2 Rt</td><td>33</td><td>3S,3L,4TL</td><td>3.8</td><td>50%</td></tr><tr><td>SD</td><td>2.00</td><td></td><td>20.17</td><td></td><td>6.31</td><td></td><td>0.73</td><td></td></tr><tr><td>Mean</td><td>15.1</td><td></td><td>119.0</td><td>3.7 Rt</td><td>33.63</td><td>2.6S,4.3 L,4TL</td><td>3.7</td><td>53%</td></tr></table>
$$
Wt = weight.
$$
$$
Side = curve side.
$$
Size = Cobb angle of lumbar or thoracolumbar curve.
Type = Curve type: S = "S" or "Inverted S" curve, L = lumbar, TL = thoracolumbar.
$R\# =$ Risser number.
$$
FHx = Positive family history
$$
Group 1 had 1 dropout, with two dropouts in both Groups 2 and 3 that were non-compliant at second or third X-rays. Three prospective patients experienced injection anxiety after randomization but before any treatment was initiated and therefore were not treated or included in the study. There were no reported injuries from the yoga pose in any group beyond a few days of sore shoulder and forearm muscles: one patient in Group 2 and one in Group 3 had transient complaints of this nature. These two patients continued the side planks on their forearms, but they did not otherwise alter their yoga routines. There were no changes in vital signs or later side-effects after administration of incobotulinum or placebo.
With rarely missed days, all patients reported performing the side plank or full plank at least twice daily beginning at a mean 30 s per side plank, with a mean initial cumulative reported dose of 80 s daily and ending at a mean 73 s per side plank after 3 months, with a mean cumulative dose of 160 s daily, during the three month period. Most participants performed the multiple side planks successively in the morning.
Mean lumbar scoliosis at study onset: Group1: $29.8^{\circ}$ (S.D. 6.68), range: $25^{\circ} - 45^{\circ}$; Group 2: $38.1^{\circ}$ (S.D. 6.52), range: $25^{\circ} - 45^{\circ}$; Group 3: $33.2^{\circ}$ (S.D. 6.7), range: $25^{\circ} - 45^{\circ}$. Mean 3-week Cobb measurements were Group 1: $30.15^{\circ}$ (S.D. 6.73.); Group 2: $29.4^{\circ}$ (S.D. 9.19); Group 3: $24.0^{\circ}$ (S.D. 8.3). The three groups were roughly equivalent at study onset. (See table 2.) Cobb measurements at 3 months were Group 1: $31.6^{\circ}$ (S.D.
7.08); Group 2: $30.35^{\circ}$ (S.D. 11.52) and Group 3: 21.0(S.D. 8.3).
Significant differences appeared between Groups 1 and 3 at three weeks $(p < 0.001)$ and at 3 months $(p < 0.001)$; between Groups 1 and 2 at 3 weeks $(p < 0.001)$ and 3 months $(p < 0.001)$. Group 3 was clinically significantly improved vs. Group 2 at 3 months $(p =.056)$. (See tables 2 and 3 and figures2, 3 and 4.)
Table 2: Study Results
<table><tr><td></td><td colspan="6">Group</td></tr><tr><td></td><td colspan="2">1</td><td colspan="2">2</td><td colspan="2">3</td></tr><tr><td></td><td colspan="2">(N = 10)</td><td colspan="2">(N = 10)</td><td colspan="2">(N = 10)</td></tr><tr><td>Variable</td><td>mean</td><td>sd</td><td>mean</td><td>sd</td><td>mean</td><td>sd</td></tr><tr><td>Age (yrs)</td><td>16.0</td><td>2.4</td><td>16.8</td><td>2.8</td><td>15.8</td><td>2.0</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Weight (lbs)</td><td>119.3</td><td>13.7</td><td>117.5</td><td>20.2</td><td>126.7</td><td>13.0</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Risser</td><td>3.9</td><td>0.9</td><td>3.6</td><td>1.3</td><td>3.7</td><td>0.7</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Male sex (%)</td><td>0.30</td><td></td><td>0.30</td><td></td><td>0.10</td><td></td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Score_T1</td><td>29.8</td><td>6.6</td><td>37.5</td><td>8.0</td><td>33.2</td><td>6.7</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Score_T2</td><td>30.2</td><td>6.2</td><td>28.8</td><td>10.2</td><td>24.0</td><td>8.3</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Score_T3</td><td>31.6</td><td>6.4</td><td>29.8</td><td>12.7</td><td>21.0</td><td>9.2</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Change Score T2 minus T1</td><td>0.4</td><td>1.6</td><td>-9.1</td><td>5.8</td><td>-9.2</td><td>5.8</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Change Score T3 minus T1</td><td>1.8</td><td>2.5</td><td>-7.8</td><td>7.3</td><td>-12.2</td><td>5.2</td></tr></table>
Table 3: Regression Results
<table><tr><td>Time Points</td><td></td><td colspan="3">Comparison of Group 2 vs. Group 1</td><td colspan="3">Comparison of Group 3 vs. Group 1</td><td colspan="3">Comparison of Group 3 vs. Group 2</td></tr><tr><td></td><td></td><td>Beta</td><td>se</td><td>p-value</td><td>Beta</td><td>se</td><td>p-value</td><td>Beta</td><td>se</td><td>p-value</td></tr><tr><td>T2 minus T1</td><td>Crude</td><td>-9.1</td><td>2.2</td><td>< 0.001</td><td>-9.6</td><td>2.2</td><td>< 0.001</td><td>-0.4</td><td>2.0</td><td>0.85</td></tr><tr><td></td><td>\(Adjusted {}^{a} \)</td><td>-0.3</td><td>2.5</td><td>0.001</td><td>-9.9</td><td>2.5</td><td>< 0.001</td><td>-0.6</td><td>2.7</td><td>0.83</td></tr><tr><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>T3 minus T1</td><td>Crude</td><td>-9.6</td><td>2.4</td><td>< 0.001</td><td>-14.0</td><td>2.4</td><td>< 0.001</td><td>-4.5</td><td>2.4</td><td>0.076</td></tr><tr><td></td><td>\(Adjusted {}^{a} \)</td><td>-9.4</td><td>2.7</td><td>0.002</td><td>-15.1</td><td>2.6</td><td>< 0.001</td><td>-5.7</td><td>2.8</td><td>0.056</td></tr></table>
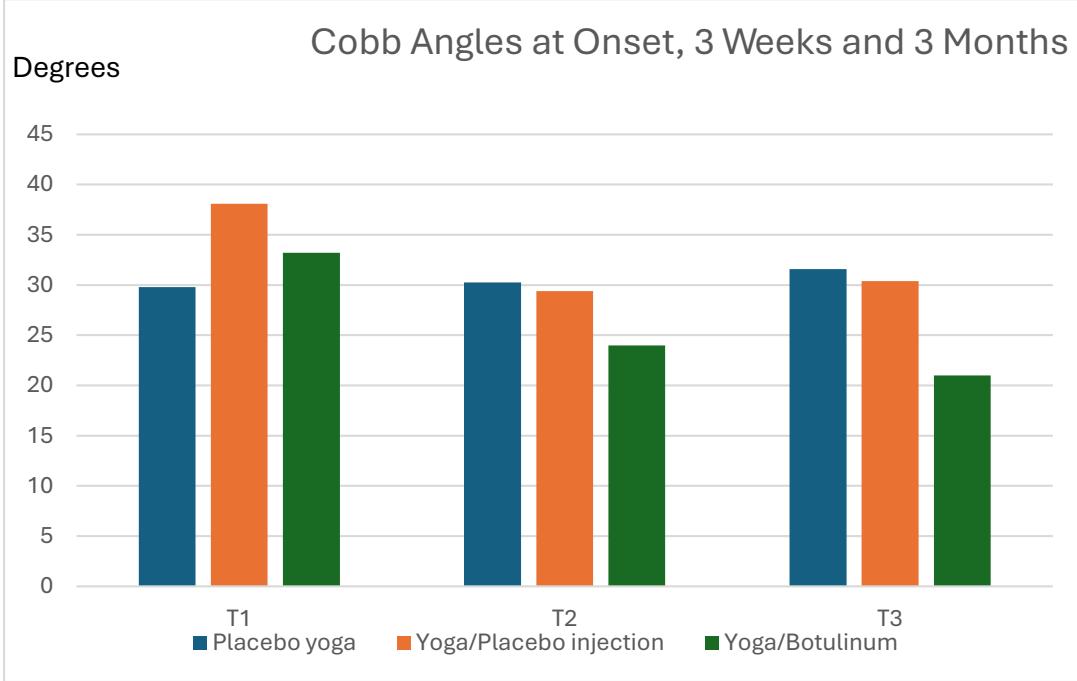
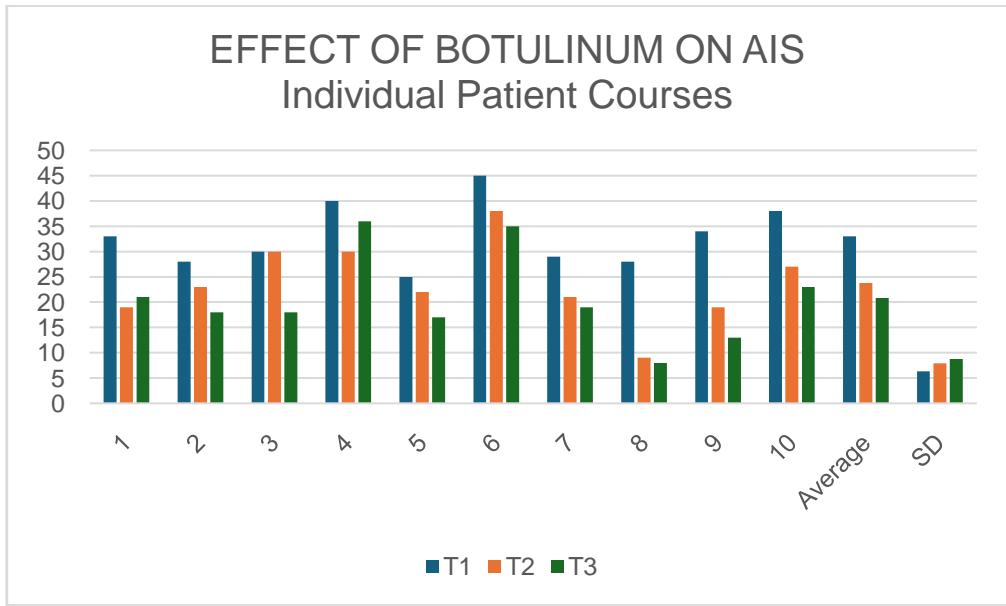
Figure 2: Greatest Reductions with Yoga and Botulinum Figure 3: T1 = Study onset T2 = 3 weeks later. T3 = 3 months later. The magnitude of individual curve improvement: Group 1 (left-most columns) placebo yoga, Group 2 (middle column) true yoga pose and placebo injection, and Group 3 (right-most columns) true yoga pose and botulinum injection into the concave side's paraspinal musculature, the quadratus lumborum and the psoas muscles
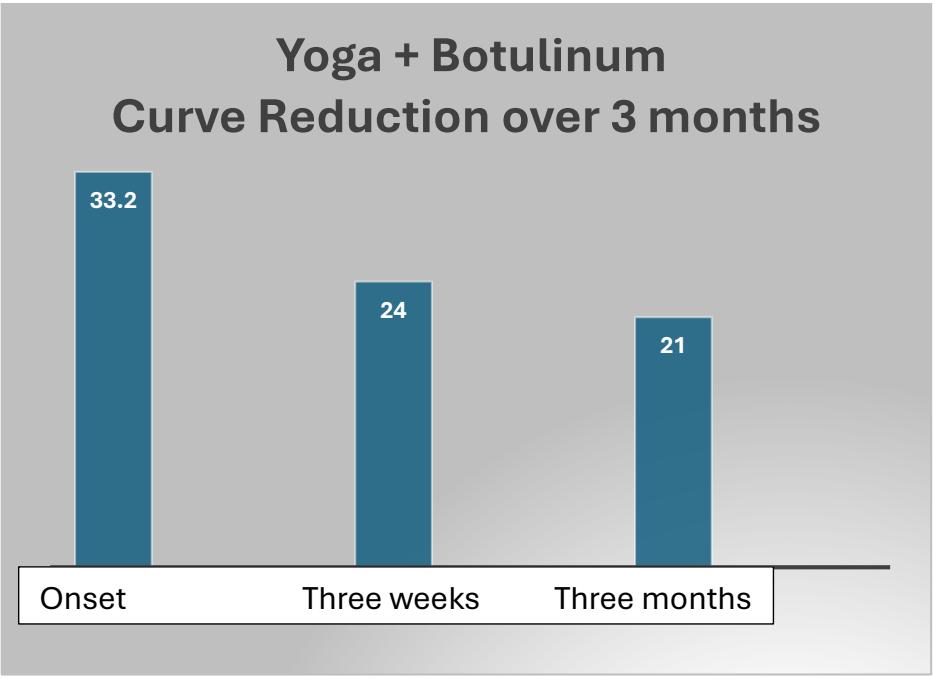
Figure 4: Mean curve reduction in Group 3 over 3 months = 36.75%
Apart from the transiently sore shoulders and forearms mentioned above, no harms were seen in any participants, although they were rigorously sought along SOSORT guidelines.[13]
## IV. DISCUSSION
The data, results and implications of this small study must be regarded with caution.[32] We view the spine as a tensegrity structure, a concept of the architect Buckminister Fuller which embraces configurations known for their strength and dynamic response to load,[34] like the human spine. Tensegrity structures are not held together by nails or rivets but by tension between their parts. Tent poles, Roman arches and radio antennae with their supporting cables are examples. The solar system, and the Bohr atom are somewhat extended examples, with gravity and centrifugal force, and electrical charges force providing the invisible tethers that generate tension and retain the structures' integrity. The spine may be seen as such a structure, but unlike the static edifices of architecture, the spine is held together by the quite variable tensions of the muscles that surround it. A spine-like tower by Frei Otto, Vertebras Tensadas, which curves in response to pressure from its cables is an architectural example of this. Seen this way, pervasive muscular asymmetry could be a major aspect of scoliosis.
Throughout the phylum Chordata, the spinal cord and the notochord are composed of many segments or metameres. These elementary units are interrelated in their control and in their movements and comprise a basic defining characteristic of the phylum. The spinal cord and its attendant ligaments, and, critically, its muscular attachments, always allow for movement and changes in leverage in all three planes, although this differs greatly from, e.g., thoracic to lumbar spine. In the turtle, it is the ribs that have coalesced to form the shell; inside it is a segmented creature with a flexible spine. To the authors' knowledge, in no case does a single bone form the spine the way the femur forms the sole support in the thigh. Throughout the phylum, from reptiles to humankind, the spine is always firm, but flexible in its multiple vertebrae, giving support, balance and leverage to our various bending, twisting, liftings and inclinations. However, many of the prominent surgeries of our day fuse the spine, rendering portions of it inelastic in a way nature has never allowed. An alternative therapy that repairs the spine without fixing it in a set conformation would be advantageous.
Significant improvement in Cobb angles at three weeks post-botulinum-injection in Groups 2 and 3 vs. Group 1 supports the hypothesis that some AIS is due at least in part to muscular imbalance, and that efforts to strengthen the convex muscles and temporarily weaken the concave muscles reverse the scoliosis significantly. Previous work with children with cerebral palsy had been ineffective and possibly dangerous,[25] but EMG work with children having AIS reveals that botulinum toxin alters side-to-side muscle recruitment ratios.[36] The simultaneous use of yoga and incobotulinum seems to have several advantages even after the two-month period of the medicine's activity:
1) Although inactive after two months, longer-term reduction in muscle tension is seen in botulinum toxin's cosmetic and dental uses.[37-41]
2) The botulinum weakens the strong (concave) side of the lumbar curve, enabling the actin and myosin fibers of the weak (convex) side to slide further together, increasing the number of cross bridges, and proportionately increasing their power to contract.[42]
3) Three-times-daily practice of the side plank yoga pose alone, held for as long as possible once daily, has been shown[27-29] to reverse lumbar curves due to AIS, through its strengthening effect on muscles of the convex side of the lumbar curve during the three-month period. The "head start" given by the incobotulinummay raise patients' enthusiasm, a critical ingredient in maximal compliance.
The adolescent idiopathic scoliotic spine is vulnerable to severe deepening of its curve. This is evidenced in the dramatic increase in Cobb angles seen in some patients. This may suggest that the actual advantage of the incobotulinum-plus-side-plank program may be even greater than those seen in this study of adolescents. This tendency of AIS to worsen dramatically in the teen years may to some extent obscure the actual benefit that intervention group patients received regarding the corrective influence of the yoga plus botulinum injections.
If the efficacy of this method is borne out in larger studies, it is sufficiently innocuous, low-cost and readily available to enable young people and their parents to embark on treatment of lumbar and thoracolumbar AIS as it develops, and before it reaches anatomically and socially significant levels.
## V. LIMITATIONS OF THE STUDY
1) Although it reached statistical significance, this randomized controlled study is based on a small sample. Larger, randomized controlled trials are clearly necessary to demonstrate the efficacy of the botulinum-plus-yoga treatment more reliably.
2) A single blinded radiological opinion was utilized throughout this study. A second and even a third blinded radiologist (for non-unanimous assessments) would improve the objectivity in these studies.
3) The opposite limitation is also present: the ranges of the patients' Risser numbers, ages and curve sizes are too large. Some researchers find that a combination of bracing and exercise is differentially effective in AIS at different Risser numbers and this type of variability may apply to the current study's treatment as well $^{4-6}$ and should be investigated.
4) Studies have found that bracing plus exercise substantially improve curves in AIS. ${}^{43}$ Studies using bracing and exercise, including the side plank and botulinum toxin injections, might further advance and enhance conservative treatment.
5) Further study design can also raise the level of objectivity regarding harms, e.g., by measuring activities of daily living.44 More specific considerations mentioned by leaders in the field may also be relevant, including aesthetics, quality of life, disability, back pain, psychological well-being, self-esteem, body image and embarrassment in high school.13,14
6) Longer follow-up is also necessary to demonstrate the value of the treatment. Two- or three-year follow-up or more would be desirable.
7) This study injected the minimal effective doses of botulinum. Dosages up to six times greater are patently safe.[45] It is possible that a proportionately greater effect would be seen with larger doses of incobotulinum. This study does not answer that important question.
8) One may additionally question whether the most relevant muscles have been treated. The iliocostalis, longissimus, semispinalis and spinalis muscles, as well as the external and internal intercostals and obliques, the superior and inferior serratus posterior, the subcostal, the quadratus lumborum, the latissimus dorsi and trapezius, the transversus abdominis, the rectus abdominis and the diaphragm itself might all function to laterally flex and/or rotate the spine. These muscles should be studied, both with EMG and possibly musculoskeletal ultrasound in different exercises and other types of exertion vis à vis strengthening them, and for appropriate dosages of botulinum toxin to weaken their contralateral counterparts.
## VI. CONCLUSIONS
Muscular imbalance appears to play a part in the pathogenesis and longevity of adolescent idiopathic lumbar scoliosis. The side plank and botulinum toxin type A injections may be more effective in reversing lumbar AIS than a placebo yoga pose.
Funding
This study was funded by Merz Pharmaceuticals and registered with ClinicalTrials.org at NCT04922983 on 17 July 2021. Travel to and from our office was partially subsidized by the Childrens Scoliosis Foundation of California.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the institutional Review Board CIRBI, currently Advarra on December 2, 2020, approval number "The IRB approved the above referenced protocol and the site with the modifications listed below on 28 May 2021: Modifications to the Adult/Parent/Subjects turning Age of Majority (AOM) Informed Consent Form".
### Informed Consent Statement
Written informed consent was obtained from all subjects involved in this study. In the case of minors, written informed consent was obtained from their parents or guardians.
#### Data Availability Statement
The data for this study can be found at Figshare.
#### Conflicts of Interest
#### ACKNOWLEDGEMENTS
The authors acknowledge the able assistance of Anne Knox, Dr. Faisal Adjei, Gabriel Ntow Quao, Ph.D and the Childrens Scoliosis Foundation of California and the Childrens Scoliosis Foundation of Ghana.
Generating HTML Viewer...
References
47 Cites in Article
S Sung,H Chae,Lee (2021). Incidence and Surgery Rate of Idiopathic Scoliosis: A Nationwide Database Study.
M Konieczny,H Senyurt,R Krauspe (2013). Epidemiology of adolescent idio pathic scoliosis.
B Longworth,R Fary,D Hopper (2014). Prevalence and predictors of adolescent idiopathic scoliosis in adolescent ballet dancers.
Hee-Kit Wong,Ken-Jin Tan (2010). The natural history of adolescent idiopathic scoliosis.
L Ragborg (2022). Long term curve progression in idiopathic scoliosis: 40-year follow-up.
Alastair Stirling,Denise Howel,Peter Millner,Safaʼa Sadiq,David Sharples,Robert Dickson (1996). Late-Onset Idiopathic Scoliosis in Children Six to Fourteen Years Old. A Cross-Sectional Prevalence Study*.
A Nachemson,L Peterson (1995). Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society..
Manuel Rigo,Mónica Villagrasa,Dino Gallo (2010). A specific scoliosis classification correlating with brace treatment: description and reliability.
Christine Coillard,Alin Circo,Charles Rivard (2014). SpineCor treatment for Juvenile Idiopathic Scoliosis: SOSORT award 2010 winner.
Stuart Weinstein,Lori Dolan,James Wright,Matthew Dobbs (2013). Effects of Bracing in Adolescents with Idiopathic Scoliosis.
Angelo Aulisa,Vincenzo Guzzanti,Francesco Falciglia,Marco Giordano,Emanuele Marzetti,Lorenzo Aulisa (2015). Lyon bracing in adolescent females with thoracic idiopathic scoliosis: a prospective study based on SRS and SOSORT criteria.
S Negrini,G Marchini (2007). Efficacy of the symmetric, patient-oriented, rigid, three-dimensional, active (SPoRT) concept of bracing for scoliosis: A prospective study of the Sforzesco versus Lyon brace.
Stefano Negrini,Sabrina Donzelli,Angelo Aulisa,Dariusz Czaprowski,Sanja Schreiber,Jean De Mauroy,Helmut Diers,Theodoros Grivas,Patrick Knott,Tomasz Kotwicki,Andrea Lebel,Cindy Marti,Toru Maruyama,Joe O’brien,Nigel Price,Eric Parent,Manuel Rigo,Michele Romano,Luke Stikeleather,James Wynne,Fabio Zaina (2016). 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth.
Traci Schwieger,Shelly Campo,Stuart Weinstein,Lori Dolan,Sato Ashida,Keli Steuber (2016). Body Image and Quality-of-Life in Untreated Versus Brace-Treated Females With Adolescent Idiopathic Scoliosis.
Bin Wang,Yue Sun,Xiaoqi Guo,Jiangang Cao,Haoyuan Lu,Wei Chen,Jie Chen,Qian Zhu,Chong Zhang,Ming Zhang,Feilong Zhu (2022). The efficacy of 3D personalized insoles in moderate adolescent idiopathic scoliosis: a randomized controlled trial.
Gozde Yagci,Yavuz Yakut (2019). Core stabilization exercises versus scoliosis-specific exercises in moderate idiopathic scoliosis treatment.
Sanja Schreiber,Eric Parent,Douglas Hedden,Marc Moreau,Doug Hill,Edmond Lou (2014). Effect of Schroth exercises on curve characteristics and clinical outcomes in adolescent idiopathic scoliosis: protocol for a multicentre randomised controlled trial.
G Tian,M Shen,W Jiang (2015). Case-control study on spinal leveraging manipulation and medicine for the treatment of degenerative scoliosis.
Hikmet Kocaman,Nilgün Bek,Mehmet Kaya,Buket Büyükturan,Mehmet Yetiş,Öznur Büyükturan (2021). The effectiveness of two different exercise approaches in adolescent idiopathic scoliosis: A single-blind, randomized-controlled trial.
S Seki,M Iwasaki,H Makino (2022). Association of Ligamentum Flavum Hypertrophy with Adolescent Idiopathic Scoliosis Progression-Comparative Microarray Gene Expression Analysis.
Min-Rou Lin,Po-Hsin Chou,Kuei-Jung Huang,Jafit Ting,Chia-Ying Liu,Wan-Hsuan Chou,Gan-Hong Lin,Jan-Gowth Chang,Shiro Ikegawa,Shih-Tien Wang,Wei-Chiao Chang (2023). Whole-Exome Sequencing Identifies Genetic Variants for Severe Adolescent Idiopathic Scoliosis in a Taiwanese Population.
Irene Cortés-Pérez,Lourdes Salamanca-Montilla,Francisca Gámiz-Bermúdez,Esteban Obrero-Gaitán,Alfonso Ibáñez-Vera,Rafael Lomas-Vega (2023). Vestibular Morphological Alterations in Adolescent Idiopathic Scoliosis: A Systematic Review of Observational Studies.
Nicola Montemurro,Luca Ricciardi,Alba Scerrati,Giorgio Ippolito,Giorgio Lofrese,Sokol Trungu,Andrea Stoccoro (1925). The Potential Role of Dysregulated miRNAs in Adolescent Idiopathic Scoliosis and 22q11.2 Deletion Syndrome.
Vaiva Seleviciene,Aiste Cesnaviciute,Birute Strukcinskiene,Ludmiła Marcinowicz,Neringa Strazdiene,Agnieszka Genowska (2022). Physiotherapeutic Scoliosis-Specific Exercise Methodologies Used for Conservative Treatment of Adolescent Idiopathic Scoliosis, and Their Effectiveness: An Extended Literature Review of Current Research and Practice.
Oliver Hausmann,Thomas B�ni,Christian Pfirrmann,Armin Curt,Kan Min (2003). Preoperative radiological and electrophysiological evaluation in 100 adolescent idiopathic scoliosis patients.
Izabela Skibinska,Marek Tomaszewski,Miroslaw Andrusiewicz,Paulina Urbaniak,Roza Czarnecka-Klos,Milud Shadi,Tomasz Kotwicki,Malgorzata Kotwicka (2016). Expression of Estrogen Receptor Coactivator Proline-, Glutamic Acid- and Leucine-Rich Protein 1 within Paraspinal Muscles in Adolescents with Idiopathic Scoliosis.
Loren Fishman,Erik Groessl,Karen Sherman (2014). Serial Case Reporting Yoga for Idiopathic and Degenerative Scoliosis.
Loren Fishman,Erik Groessl,Paul Bernstein (2017). Two Isometric Yoga Poses Reduce the Curves in Degenerative and Adolescent Idiopathic Scoliosis.
Jingyuan Zhang,Ling Li (2021). Analysis of Treatments of Adolescent Idiopathic Scoliosis.
Natalya Sarkisova,Lindsay Andras,Joshua Yang,Tracy Zaslow,Bianca Edison,Vernon Tolo,David Skaggs (2019). Side Plank Pose Exercises for Adolescent Idiopathic Scoliosis Patients.
Loren Fishman (2021). Side Plank Pose Exercises for Adolescent Idiopathic Scoliosis Patients—Some Concerns About a Randomized Controlled Trial.
Daniela Junqueira,Liliane Zorzela,Susan Golder,Yoon Loke,Joel Gagnier,Steven Julious,Tianjing Li,Evan Mayo-Wilson,Ba Pham,Rachel Phillips,Pasqualina Santaguida,Roberta Scherer,Peter Gøtzsche,David Moher,John Ioannidis,Sunita Vohra (2022). CONSORT Harms 2022 statement, explanation, and elaboration: updated guideline for the reporting of harms in randomised trials.
Stefano Negrini,Salvatore Atanasio,Claudia Fusco,Fabio Zaina (2023). Effectiveness of complete conservative treatment for adolescent idiopathic scoliosis (bracing and exercises) based on SOSORT management criteria: results according to the SRS criteria for bracing studies - SOSORT Award 2009 Winner.
B Fuller (2020). CetraRuddy Architecture, New York, NY, USA ARO, New York, NY, USA.
Christian Wong,Søren Pedersen,Billy Kristensen,Kasper Gosvig,Stig Sonne-Holm (1976). The Effect of Botulinum Toxin A Injections in the Spine Muscles for Cerebral Palsy Scoliosis, Examined in a Prospective, Randomized Triple-blinded Study.
Wei Wang,Jianping Huang,Jun Wang,Wanzhang Yang,Guanglin Li (2025). Effects of botulinum toxin on paraspinal muscle imbalance during spinal motions in adolescents with idiopathic scoliosis: Assessment using high-density electromyography.
Yu Kim,Oh Lim,Won Choi (2020). Are There Differences Between Intradermal and Intramuscular Injections of Botulinum Toxin on the Forehead?.
Victoria Sitnikova,Antti Kämppi,Olli Teronen,Pentti Kemppainen (2022). Effect of Botulinum Toxin Injection on EMG Activity and Bite Force in Masticatory Muscle Disorder: A Randomized Clinical Trial.
Dimos Mitsikostas,Andrzej Dekundy,Angelika Hanschmann,Michael Althaus,Astrid Scheschonka,Fernando Pagan,Joseph Jankovic (2021). Duration and onset of effect of incobotulinumtoxinA for the treatment of blepharospasm in botulinum toxin-naïve subjects.
Han-Cheng Wang,Lin-Fen Hsieh,Wen-Chou Chi,Shih-Min Lou (2002). Effect of Intramuscular Botulinum Toxin Injection on Upper Limb Spasticity in Stroke Patients.
D Hexsel,I Valente-Bezerra,G Mosena (2023). Subjective and Objective Measurements of the Facial Effects of Microdoses of Botulinum Toxin.
Ryan Colquhoun,Christopher Gai,Danielle Aguilar,Daniel Bove,Jeffrey Dolan,Andres Vargas,Kaylee Couvillion,Nathaniel Jenkins,Bill Campbell (2018). Training Volume, Not Frequency, Indicative of Maximal Strength Adaptations to Resistance Training.
Guilherme Da Silveira,Rodrigo Andrade,Gean Guilhermino,Ariane Schmidt,Lucas Neves,Ana Ribeiro (2022). The Effects of Short- and Long-Term Spinal Brace Use with and without Exercise on Spine, Balance, and Gait in Adolescents with Idiopathic Scoliosis.
Mary Law,Lori Letts (2023). A Critical Review of Scales of Activities of Daily Living.
Loren Fishman,Sarah Schmidhofer (2014). Use of botulinum neurotoxin in the treatment of piriformis syndrome.
D Truong,D Dressler,M Hallett,C Zachary,M Pathak (2023). Manual of Botulinum Toxin Therapy.
A Peterson (null). SCRIPTS: Recovering publication lists from Google Scholar profiles.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Loren Fishman. 2026. \u201cYoga and Botulinum Toxin Reduce Adolescent Idiopathic Lumbar Scoliosis – A Control, Randomized Study\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 25 (GJMR Volume 25 Issue K3): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































