
I. INTRODUCTION
Breast cancer is a diverse family of disease. It gives rise to major threat to social economy and women's health and has called attention from researchers for many years [1, 2]. Pakistan has the highest incidence rate in Asia, with approximately one in every nine women suffering from breast cancer [3]. Early and timely detection of breast cancer can bring down morbidity and mortality related with this disease process[4]. The prognosis of patients with invasive breast carcinomas can be predicted by numerous factors in which identification of metastasis in axillary lymph nodes is pivotal. It is also essential for developing appropriate treatment regimes. Axillary lymph nodes metastasis is also the key predictor of overall survival and recurrence. While the 5-year survival rate for patients with disease localized to the breast is , these numbers drop to for patients with axillary lymph nodes metastases (AXLN). Staging the axilla for the presence of axillary lymph node (LN) metastasis, the number and location of positive LNs is of prime importance, as it determines the pathologic stage of breast cancer[5-7].
Although the invasive, standard of care, surgical means of staging axilla via sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND) are critical in customizing the treatment with adjuvant chemotherapy or radiotherapy, morbidity and complications associated with these surgical procedures are exigent and require an alternate less invasive system of practice. Hence, imaging of breast and axilla via ultrasound and mammogram has already drawn interest for preoperative staging as a part of minimally invasive approaches in the investigation of the axilla [8]. Magnetic resonance imaging as an adjunct to mammography and ultrasound refines the precision of the estimate of the true magnitude of disease in the affected and contralateral breast. It also improves accuracy of depiction of multicentric disease and sonographically occult disease in axilla [9].
Recent researches have shown important imaging predictors of AXLN metastasis, i.e. tumor size, tumor quadrant, local invasion status, pathologic type, and molecular subtypes. [8-13]. In this retrospective study, we have evaluated the value of using the ultrasound and mammographic features of primary breast malignancy to predict AXLN in patients with known biopsy proven breast cancer. We also determined the impact of demographic factors and various histopathological features of breast cancer on axillary lymph nodes metastasis.
II. MATERIAL AND METHODS
a) Study population
This study was carried out at the Radiology Department of Sindh Institute of Urology and Transplantation (SIUT) Karachi. The requirement of individual informed consent for this descriptive retrospective study was waived by our institutional ethics committee.
b) Inclusion criteria
Pertinent information was collected from ultrasound and mammogram images.
Patients from both the screening and symptomatic populations.
Patients with pathologically diagnosed breast cancer.
Axillary lymph nodes status illustrated either by FNAC (Fine needle aspiration cytology), trucut biopsy or SNLBX (Sentinel lymph node biopsy).
c) Exclusion criteria
Imaging, including baseline breast and axillary ultrasounds, mammograms and histopathological analysis done outside our institution were excluded from this study.
Patients with incomplete records and unsatisfactory images.
Ductal carcinoma in situ (DCIS) were also excluded from the study.
Patients who have undergone neo-adjuvant chemotherapy.
Patients without histopathological diagnosis of axillary lymph nodes.
Bilateral breast cancers were also excluded from the study because of very few cases of bilateral breast cancers.
In this way, data from 354 patients with breast cancer were retrospectively collected between March 2021 and August 2022.
d) Ultrasound
All breast and axillary ultrasound examinations were not done under research study settings and were carried out according to the standard of care protocol, in accordance with ACR practice parameters for the performance of a breast ultrasound examination (revised 2016) [14] as a routine practice of our breast cancer unit. For sonography, Canon Xario 200 was used, with frequency of . Every ultrasound examination included both breasts and both axillary regions.
e) Digital Mammography
All mammograms were done with Selenia Dimensions 3D Digital Mammography Tomosynthesis System (Hologic, Bedford, MA, USA). Images were reviewed on high-resolution workstations. These were performed according to ACR practice parameters for the performance of screening and diagnostic mammography (revised 2018) [15]. Two standard views (craniocaudal CC and mediolateral oblique MLO) were performed as per usual for all patients. Accessory views were taken where required.
f) Ultrasound and Digital Mammogram Assessment
All ultrasound and mammogram images were reviewed by 1 of 3senior consultant radiologist in breast imaging with at least 5 years of experience each, in breast imaging. In the case of discrepancies, aconsensus was reached after discussion. The sonographic and mammographic characteristics of the breast carcinomas and axillary lymph nodes were evaluated based on the standard criteria of Breast Imaging Reporting and Data System (BIRADS). For mammogram, the features that were assessed were enumerated in Table 2 and Table 3.For ultrasound, thefeatures of primary breast malignancy and axillary lymph nodes were itemized in Table 2 and Table 4.
Data on patient's demographics and tumor characteristics, diagnostic work-up, and histopathological outcome of the axillary lymph nodes were retrospectively collected. Tissue sampling ofaxilla was performed in case of suspicious axillary lymph node(s). It was done either by core needle technique by using 18 gauge core needle, or by FNAC (when core needle biopsy was technically difficult).
Mammography has lower sensitivity for imaging of axilla because most of the axilla is pushed out of the image field after compression, even in dedicated axillary tail views of mammogram. Ultrasound is reported to be convincing examination used routinely in evaluation of lymph node involvement [4], therefore most suspicious looking lymph node on the basis of ultrasound features was selected for tissue sampling.
g) Biomarker status of the breast mass
Histopathological evaluation was done to assess morphological type of breast cancer and immunohistochemical analysis was also done on breast mass to assess ER, PR, Ki-67 index, and Her-2 neu expression. ER and PR were regarded as positive if at least of the tumor nuclei were positively stained [10]. An additional fluorescence in situ hybridization (FISH) was analyzed to detect Her-2 positivity with scores of 2 or higher. Scores of 1 or 0 were defined as Her-2 negative [10]. Ki-67 index was considered as high and was considered as low expression.
h) Statistical analysis
All the data was entered and analyzed in SPSS version 22.0. Mean and standard deviations were computed for continuous variables and categorical variables were presented as frequency and percentages and their comparison was done using bivariate Chi-square test. Multivariate binary logistic analysis was used to quantify the relative contribution of each imaging feature. P-value was considered as significant. Odds ratios and confidence intervals were recorded for predictors of AXLN metastases.
III. RESULTS
a) Demographics and AXLN metastases: (Table1)
In our data set, the median age of patients were 48.0 (+/- 11.3 S.D), out of which the majority of cancers were detected in 20-45 years of age. Among 354 patients (n=220, 62.1%) have axillary lymph node metastases (AXLN) metastases. (n=134, 37.9%) have biopsy proven benign lymph nodes. On ultrasound axilla (n= 144) show benign morphology. Among these benign looking lymph nodes (n= 66, 45.8%) turned out be malignant. (n= 78, 54.2%) share same benign morphology on histopathology as well. (n=148) are of intermediate suspicion. Among these (n= 118, 79.7%) were malignant and (n = 30, 20.3%) were benign. Among (n=62) malignant looking lymph nodes (n=36, 58.1%) were truly malignant on biopsy.
Most common complaint was lump (n=322), followed by pain (n= 20), both lump and pain (n= 6) and nipple discharge (6). Patient's age, complaints, side of tumor, family history and menopausal status did not show correlation with AXLN status.
| Demographics | Total (n = 354) | Metastatic *AXLN (n = 220) (%) | Non-metastatic *AXLN (n =134) (%) | p-value |
| Age | 0.7 | |||
| 20 - 45 | 162 | 102 (63.0%) | 60 (37.0%) | |
| 46 - 50 | 52 | 34 (65.4%) | 18 (34.6%) | |
| 50 above | 140 | 84 (60.0%) | 56 (40.0%) | |
| Complaints | 0.09 | |||
| lump | 322 | 204 (63.4%) | 118 (36.6%) | |
| lump and pain | 6 | 4 (66.7%) | 2 (33.3%) | |
| nipple discharge | 6 | 4 (66.7%) | 2 (33.3%) | |
| Only pain | 20 | 8 (40.0%) | 12 (60.0%) | |
| Side | 0.2 | |||
| Right | 182 | 118 (64.8%) | 64 (35.2%) | |
| Left | 172 | 102 (59.3%) | 70 (40.7%) | |
| Family History | 0.1 | |||
| Yes | 122 | 70(57.4%) | 52 (42.6%) | |
| No | 232 | 150(64.7%) | 82 (35.3%) | |
| Lactation history | 0.04 | |||
| Yes | 282 | 168 (59.6%) | 114 (40.4%) | |
| No | 72 | 52 (72.2%) | 20 (27.8%) | |
| Menopause | 0.2 | |||
| Yes | 182 | 118 (64.8%) | 64 (35.2%) | |
| No | 172 | 102 (59.3%) | 70 (40.7%) | |
| AXLN on ultrasound | <0.01 | |||
| Benign | 144 | 66 (45.8%) | 78 (54.2%) | |
| Intermediate suspicious | 148 | 118 (79.7%) | 30 (20.3%) | |
| Malignant | 62 | 36 (58.1%) | 26 (41.9%) |
b) Imaging findings on ultrasound and mammogram and AXLN metastases: (Table 2, 3 and 4)
Size, shape and margins of the tumor on ultrasound and digital mammogram exhibited notable association with presence of metastases in AXLN. Irregular shape (n=318) and irregular/spiculated margins (n= 315) are significantly related to presence of metastatic axillary lymph nodes (n=204, 64.2%) and (n=202, 64.1%) respectively. All tumors with circumscribed margins (n= 6) have benign lymph nodes (n= 6, 100%). We studied that AXLN metastases are more commonly found in large size of invasive breast cancer. In tumors larger than 5cm (n=144), 116(80.6%) have malignant lymph nodes, and tumors less than 2 cm (22) have only (n=8, 36.4%) positive AXLN. Posterior features of breast malignancy also expressed positive trend. Posterior acoustic shadowing (n=86) have highest percentage of metastatic AXLN (n= 64, 74.4%). Rest of the ultrasound feature of breast mass i.e. echogenicity, orientation and boundary are not correlated with AXLN metastases.
Global asymmetry in the breast also unveiled positive association. patients have globally enlarged edematous breast and (n= 50, 71.4%) have AXLN metastases. In globally small shrinking breasts (n= 10), (n= 4, 40.0% have metastases and (n=6, 60.0%) have benign lymph nodes. In our study, finding of diffuse skin thickening along with blurring of subcutaneous fat planes (n= 58) has noteworthy link. All of these patients have AXLN metastases.
BIRADS V show more significant association with positive AXLNs than BIRADS IV. In BIRADS V (n= 60), (n = 44, (73.3%) have positive AXLN and only (n=16, 26.7%) have LNs with benign findings. No association is found with multifocality/multicentricity of the breast tumors.
In our study positive correlation of breast density has also been demonstrated. Dense breasts (Type B, n= 124) and (Type C, n= 184) are associated more with the presence of AXLN metastases (n= 80, 64.5%) and (n= 126, 68.5%) respectively. Type A (n= 46) showed high percentage of (n=32, 69.6%) nonmetastatic LNs.
| Imaging findings | Total (n=354) | Metastatic *AXLN (n=220) (%) | Non-metastatic *AXLN (n=134) (%) | p-value |
| Size | ||||
| <2cm | 22 | 8 (36.4%) | 14 (63.6%) | 0.00 |
| 2-5cm | 188 | 96 (51.1%) | 92 (48.9%) | |
| >5cm | 144 | 116 (80.6%) | 28 (19.4%) | |
| Shape | 0.06 | |||
| Oval | 28 | 12 (42.9%) | 16 (57.1%) | |
| Round | 8 | 4 (50.0%) | 4 (50.0%) | |
| Irregular | 318 | 204 (64.2%) | 114 (35.8%) | |
| Margins | 0.04 | |||
| Circumscribed | 6 | 0 (0.0%) | 6 (100.0%) | |
| Microlobulated | 33 | 18 (54.5%) | 15 (45.5%) | |
| Irregular/spiculated | 315 | 202 (64.1%) | 113 (35.9%) | |
| Architectural distortion/Trabecular thickening | 0.4 | |||
| Yes | 312 | 192(61.5%) | 120 (38.5%) | |
| No | 42 | 28 (66.7%) | 14 (33.3%) | |
| Multifocality/Multicentricity | 0.9 | |||
| Yes | 58 | 36 (62.1%) | 22 (37).9% | |
| No | 296 | 184 (62.2%) | 112(37.8%) | |
| Asymmetry | 0.03 | |||
| No | 258 | 160 (62.0%) | 98 (38.0%) | |
| Global- small | 10 | 4 (40.0%) | 6 (60.0%) | |
| Global- Enlarged | 70 | 50 (71.4%) | 20 (28.6%) | |
| Focal | 16 | 6 (37.5%) | 10 (62.5%) | |
| Skin | <0.01 | |||
| Not involved | 245 | 134 (54.7%) | 111 (45.3%) | |
| Focal dimpling | 30 | 16 (53.3%) | 14 (46.7%) | |
| Diffuse thickening | 21 | 12(57.1%) | 9 (42.9%) | |
| Diffuse thickening + blurring of subcutaneous fat | 58 | 58 (100.0%) | 0 (0.0%) | |
| BIRADS | 0.01 | |||
| III | 8 | 2 (25.0%) | 6 (75.0%) | |
| IV | 252 | 146 (57.9%) | 106 (42.1%) | |
| V | 60 | 44 (73.3%) | 16 (26.7%) | |
| VI | 34 | 28 (82.4%) | 6 (17.6%) |
| Imaging findings | Total (n=354) | Metastatic *AXLN (n=220) (%) | Non-metastatic *AXLN (n= 134) (%) | p-value |
| Breast density | 0.00 | |||
| A | 46 | 14 (30.4%) | 32 (69.6%) | |
| B | 124 | 80 (64.5%) | 44 (35.5%) | |
| C | 184 | 126 (68.5%) | 58(31.5%) | |
| D | 0 | 0 | 0 | |
| Microcalcifications | ||||
| None | 282 | 166 (58.9%) | 116 (41.1%) | 0.01 |
| Within the mass | 60 | 42 (70.0%) | 18 (30.0%) | |
| Outside the mass | 2 | 2 (100.0%) | 0 (0.0%) | |
| Both within and outside the mass | 10 | 10 (100.0%) | 0 0.0% |
| Ultrasound Only | Total | Metastatic *AXLN | Non-metastatic *AXLN | p-value |
| Echo pattern | ||||
| Anechoic | 2 | 0 (0.0%) | 2 (100.0%) | |
| Hypoechoic | 306 | 186 (60.8%) | 120 (39.2%) | |
| Hyper echoic | 4 | 4 (100.0%) | 0 (0.0%) | 0.06 |
| Iso echoic | 4 | 4 (100.0%) | 0 (0.0%) | |
| Complex | 38 | 26 (68.4%) | 12 (31.6%) | |
| Posterior features | ||||
| Enhancement | 46 | 30 (65.2%) | 16 (34.8%) | |
| Shadowing | 86 | 64 (74.4%) | 22 (25.6%) | |
| Both | 216 | 126 (58.3%) | 90 (41.7%) | 0.01 |
| None | 6 | 0 (0.0%) | 6 (100.0%) | |
| Orientation | ||||
| Parallel | 60 | 40 (66.7%) | 20 (33.3%) | 0.5 |
| Anti-parallel | 280 | 170 (60.7%) | 110 (39.3%) | |
| Cannot be assessed | 14 | 10 (71.4%) | 4 (28.6%) | |
| Boundary | ||||
| Abrupt | 188 | 116 (61.7%) | 72 (38.3%) | 0.7 |
| Echogenic halo | 164 | 104 (63.4%) | 60 (36.6%) | |
c) Histopathological characteristics of breast malignancy and AXLN metastases: (Table 5)
In our study grade of invasive breast cancer and lymphovascular invasion (LVI) showed positive correlation with the presence of AXLN metastases. All grade II and III tumors and respectively, are associated with malignant LNs. On the contrary, grade I tumors showed non-malignant lymph nodes. LVI is also directly proportional to the presence of metastases. Tumors that showed LVIare . Among these
have AXLN metastases. On the other hand, luminal subtypes, Ki-67 and Her-2neu show no positive linkage.
| HP | Total | Metastatic *AXLN | Non-metastatic *AXLN | p-value |
| Luminal Classification | ||||
| A | 76 | 54 (71.1%) | 22 (28.9%) | |
| B | 158 | 94 (59.5%) | 64 (40.5%) | 0.1 |
| Her-2 enrich | 64 | 42 (65.6%) | 22 (34.4%) | |
| TNBC | 56 | 30 (53.6%) | 26 (46.4%) | |
| *TNBC v/s *Non-TNBC | ||||
| TNBC | 64 | 42 (65.6%) | 22 (34.4%) | 0.5 |
| Non-TNBC | 290 | 178 (61.4%) | 112 (38.6%) | |
| Grade | ||||
| I | 154 | 20 (13.0%) | 134 (87.0%) | <0.01 |
| II | 28 | 28 (100.0%) | 0 (0.0%) | |
| III | 172 | 172 (100.0%) | 0 (0.0%) | |
| Ki-67 | ||||
| <14 | 70 | 44 (62.9%) | 26 (37.1%) | 0.6 |
| >14 | 80 | 46 (57.5%) | 34 (42.5%) | |
| >30 | 204 | 130 (63.7%) | 74 (36.3%) | |
| Her-2neu | ||||
| +ve | 198 | 124 (62.6%) | 74 (37.4%) | 0.8 |
| -ve | 156 | 96 (61.5%) | 60 (38.5%) | |
| LVI | ||||
| Presence | 242 | 170 (70.2%) | 72 (29.8%) | <0.01 |
| Absence | 112 | 50 (44.6%) | 62 (55.4%) |
d) Multivariate analysis: (Table 6)
We also performed multivariate analysis by combining imaging findings. Irregular spiculated margins of invasive breast carcinomas are strongly associated with absence of benign LNs. (OR= 2.086)(CI= 1.067 - 4.077). Combining features of tumors, like size of 2-5/5cm, posterior acoustic shadowing and irregular spiculated margins increased significantly the probability of AXLN being metastatic. . Combining imaging features of diffuse skin thickening with diffuse skin thickening and blurring of subcutaneous fat showed significant relationship with AXLN positivity. .
| Imaging Findings | Outcome variable | p-value | Odds ratio | Confidence Interval |
| Irregular spiculated margins of v/s others | AXLN metastases v/sAXLN no metastases | .032 | 2.086 | 1.067 - 4.077 |
| 2-5 / >5 cm mass + posterior acoustic shadowing | AXLN metastases v/sAXLN no metastases | 0.01 | 2.04 | 1.163 - 3.579 |
| 2-5 / >5cm mass + irregular spiculated margins | AXLN metastases v/sAXLN no metastases | .002 | 2.438 | 1.382 - 4.300 |
| 2-5/5cm + posterior acoustic shadowing + irregular spiculated margins | AXLN metastases v/sAXLN no metastases | .013 | 2.041 | 1.163 - 3.579 |
| Diffuse skin thickening +Diffuse skin thickening and blurring of subcutaneous fat | AXLN metastases v/sAXLN no metastases | .000 | 6.481 | 3.113 - 13.497 |
IV. DISCUSSION
We studied prediction of AXLN metastasis in patients with known biopsy proven breast cancer, using ultrasound and mammographic features of primary breast malignancy. We also determined the impact of demographic factors and various histopathological features of breast cancer on AXLN metastasis. We studied that size and margins of the mass on imaging, posterior features of the mass on ultrasound and involvement of skin of breast strongly correlates with AXLN metastases. Breast density on mammogram also showed positive trend. Histopathological factors that showed strong correlation with presence of AXLN metastases are tumor grade and LVI.
T stage of invasive breast cancer is represented by tumor size. It is most simple yet principal predictor for AXLN metastasis. Our study also established this finding that large tumor size has higher incidence of metastatic involvement of axilla [6]. This finding is in accordance with previous study showing that increase in tumor size has direct relationship with AXLN metastasis [13] [16] [17]. This implies the importance of early and timely detection of breast cancer [4].
Another important predictor of AXLN metastases are shape and margins of tumor. Our study showed borderline significance with shape of the tumor mass. Association of irregular shape and margins of tumor with AXLN metastases have been established in previous studies as well [5]. The shape of a tumor has some specific growth patterns, which makes it an important predictor of metastatic spread. Irregular shape of malignant tumors represent an infiltrative growth style, which is also fast growing in nature. This rapid growth pattern predisposes cancer cells to penetrate surrounding tissues, including blood vessels and lymphatic leading to axillary lymph node metastasis. Conversely, round shape of the tumor is believed to be slow growing and have benign propensity [5].
In our study, along with the size, irregular shape and irregular margins of invasive breast cancer, another important tumor characteristic serving as a predictor of LN involvement in axilla is posterior acoustic feature on ultrasound. Posterior acoustic shadow thought to arise from stromal fibrosis and desmoplastic reaction and it is a well-known feature of malignant breast masses. We postulate that relatively longer growth pattern of these tumors with posterior acoustic shadowing represent a higher risk of AXLN involvement [6] [13] [18]. Multivariate logistic regression analysis done in our study, showed strong interrelationship of tumor size 2-5/5cm, along with posterior acoustic shadowing and irregular margins/shape of the tumor with malignant AXLN. [Figure 1 (a) (b)]. In our study no correlation is found with mass boundary and orientation on sonography, however Luo et.al [1] proposed that lesion boundary and Wang et.al. [17] documented that vertical orientation was independently associated with malignant AXLN.
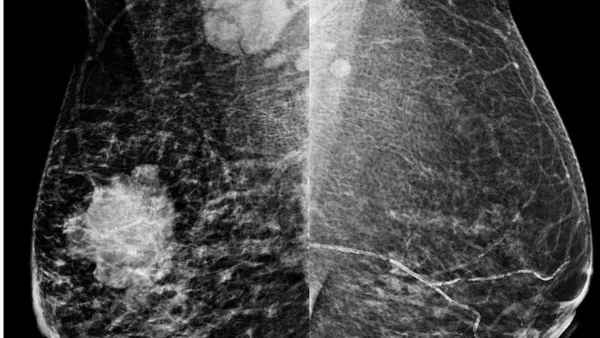
We found out that skin changes are independent predictors of malignant status of AXLN. Multivariate analysis of diffuse thickening of skin alone, along with diffuse thickening and blurring of subcutaneous fat displayed convincing positive association. Invasive breast carcinomas are known to demonstrate secondary signs of skin changes in involved breast. It can present either as direct focal retraction and adhesion of tumor with the overlying skin, or in more generalized thickening, commonly associated with presence of edema in the breast parenchyma. Edema and subcutaneous fat layer blurring are caused by the distension of blood vessels and lymphatics in the breast [19]. Some studies also showed correlation of AXLN metastases with distance of tumor from the skin [20]. Lymphovascular invasion (LVI) is another dominant histopathological predictor of AXLN metastasis. Our study also showed LVI to be an independent risk factor. Presence of lymphovascular tumor emboli is a well-founded indicator for distant metastasis and overall survival in breast cancer [19]. LVI and presence of AXLN metastases can also be correlated with the presence of diffuse thickening and blurring of subcutaneous fat on mammograms. [Figure 2 (a) (b)]. We also studied positive trend of high grade tumors with malignant AXLN. High histopathological grade represents invasiveness and are proven to be associated with more advance and aggressive disease, and showed link with extensive malignant nodal disease in axilla [1] [16] [17] [21].
We did not recognize association of morphological type of breast cancer, immunohistochemical (IHC) subtypes, Ki-67 and Her-2 status with axillary nodal status. Similarly, Shaikh S [18] had studied sono-mammometry score in prognostication of IHC subtypes of breast carcinomas, also documented no association with of IHC subtypes with nodal stage. Contrarily, Li et.al.[6]studied that pathological type of invasive breast cancer, IHC subtype and Her-2 positivity are associated with heavy nodal tumor burden. Similarly, Luo et.al [1] proposed similar kind of association of IHC markers and Ki-67 with AXLN status.
Breast density and BIRADS also demonstrated positive link with AXLN status. Dense breasts on mammogram are shown to have substantial association with malignant LNs. One explanation of this finding can be related to the younger mean age of our patient's cohort i.e. 48.0 S.D). We also speculate that dense fibroglandular parenchyma of the breast on mammogram can lead to delay in the diagnosis of invasive breast carcinomas and therefore show positive trend towards AXLN metastases. The ACR- BIRADS score is also a well approved reporting method to anticipate invasiveness of tumors. In our study BIRADS
V show more significant association with positive AXLNs than BIRADS IV, which points towards increasing aggressive behaviour with increase in BIRADS score [6].
In our study morphology of axillary lymph nodes on axillary ultrasound is strongly associated with metastatic nodal status. Lartigue et.al [22] had showed ultrasonography to be an effective modality for the detection of LN metastases. There are some suggested imaging parameters for malignant lymph nodes, which is a separate wide research area and out of the scope of this study. [Figure 3(a)(b)].
Our study has some limitations. First, our study included small numbers of patients with retrospective evaluation of data. Real time verification on ultrasound was missing. Prospective studies and increasing the sample size are needed to authenticate these results.
Strength of our study, however, includes histopathological correlation of all axillary LNs, either by percutaneous biopsy, FNAC or SNLBX.
V. CONCLUSION
Breast cancer is a heterogeneous group of disease. Early and timely detection of breast cancer has significant impact on prognosis related with this disease process. The prognosis of patients with invasive breast carcinomas can also be predicted by numerous factors in which identification of metastasis in axillary lymph nodes has important role. Sentinel lymph node biopsy, although reliable and established method in invasive breast cancer for the assessment of axillary status, there is always a need for minimally invasive examination method with less morbidity and less physical damage. Predictors of axillary lymph node metastasis by imaging characteristics of primary breast masses and its associated features provide insightful results and can become standard of care for assessment of axillary status.