## I. INTRODUCTION
Dental caries is a multifactorial bacterial process, a chronic, site-specific progressive disease process resulting from variances in the physiological imbalance between tooth structure and oral biofilm. The process initiates when the pH variation causes a drop in the mineral content of the tooth over time. It is one of the most prevalent diseases known till now. Based on an international epidemiology survey confirms that dental caries is a distinctive disease affecting children in both developed and developing countries[^3] The scenario in developing countries is deficient due to the availability of resources such as basic oral hygiene practices and the affordability of dental treatment such as restoration. Thus, unmanaged dental caries indirectly affect their general health and social well-being.[^4] For ages, caries have been managed by the mechanical removal of infected portions of the tooth followed by restoration.[^5] The choice of restoration solely depends on the operator itself, which can be based on the affordability of high-quality instruments, standard restorative materials, and advanced skills. Then, it also depends on the patient's financial status, which can compromise patient cooperation with treatment. Due to such hurdles in treating caries in the young population, operators are in a dilemma about whether to evacuate all cavitated tooth structures and provide sound restoration. Therefore, the treatment that can withhold caries progression has been pioneered in such unrecognized communities of children[^6].
Silver diamine fluoride (SDF), a fluoride-containing agent, has been proven to arrest the caries process and is known to prevent the neoformation of dental caries. As per historians, SDF's first documented use was in Japan's early 1960s-70s; its knowledge could not spread worldwide due to unassumed circumstances. Based on studies conducted in schools in China, SDF has been used since the early $21^{\mathrm{st}}$ century as an anti-cavity agent in school-going children. In various case series and studies during the first decade of the century, SDF was already known as a miraculous, effective agent that could be used to arrest caries. The well-known case series are.
1. Yee et al. in Nepal and Braga et al. in the United States conducted their studies in 2009 and documented SDF as a 'caries arresting agent' due to the extensive use in their case series and based on their follow-ups.[9,10]
2. Knight et al. in Australia, in their in-vitro studies, proved the properties of SDF as an anti-microbial and caries arresting agent, which was conducted around 2005-09. <sup>11,12</sup>
All around the world, studies have been conducted in the interest of SDF's clinical implications. Hence, this article will meticulously focus on the roots of this unhesitating agent. This will include its extensive use in preventing and arresting caries in both dentitions.
## II. HISTORY OF SILVER IN THE DENTAL WORLD
Silver has been used for generations for medical reasons dating as far back as 1000 AD. $^{13}$ SDF was developed by Reichi Yamaga, Mizuho Nishino, and colleagues to prevent and treat dental caries $^{14}$ and it has been used since its approval in 1970 by PMDA (equivalent to FDA) Japan. This was not globalized because of the language barrier; little evidence is available in English now. Around the 1980s, Australia and Brazil allowed the use of SDF, and in early 2014, the FDA approved it as a medical device to treat dental hypersensitivity. Finally, in 2016, SDF was introduced in the United States as interim caries arresting medicine, and in 2017, Canada approved SDF as a treatment for dental caries. $^{15}$
## III. PHYSICAL PROPERTIES SILVER DIAMINE FLUORIDE
SDF is a highly alkaline solution with pH = 11 to 13, depending on assorted brands, which does not require a reducing agent such as silver fluoride to make it diamine. Chemically, SDF is more stable than silver fluoride, which can be kept at a constant concentration.[16] SDF is a clear and colorless solution composed of silver's anti-bacterial and fluoride, which helps prevent the progression of caries. The fluoride concentration is 44800 ppm in SDF, the highest in any other fluoride-related product used in dentistry.[17]
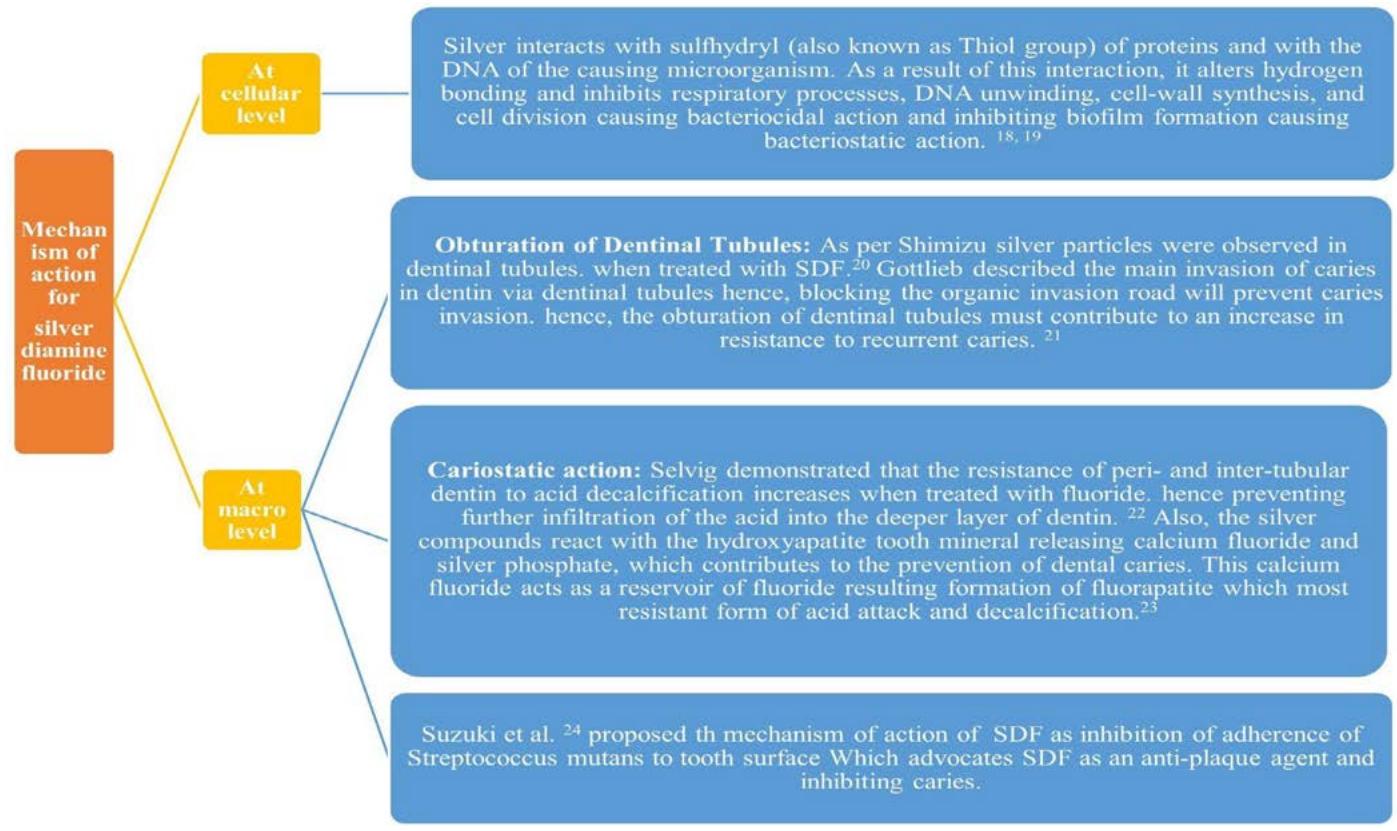
## IV. MECHANISM OF ACTION FOR SILVER DIAMINE FLUORIDE
There are mechanisms proposed for SDF. Figure 1 will emphasize the critical tool behind the working of SDF.
## V. CLINICAL IMPLICATION OF SILVER DIAMINE FLUORIDE
The following table will emphasize the use of SDF in detail, along with its documented use.
<table><tr><td>Sr no</td><td>Function</td><td></td><td>Description</td><td>Documented uses</td></tr><tr><td>1.</td><td>Preventive</td><td>a. To prevent pit and fissure caries.</td><td>The most vulnerable site for dental caries is even more susceptible than smooth surface caries due to the surface structure. The deep pits and fissures make it challenging to self-clean or rinse the surface and detect incipient decay. Studies show topical fluoride has not been beneficial in preventing such caries.</td><td>According to Sato et al. (1970)25 mentioned the effectiveness of SDF in preventing pit and fissure lesions in the first molar and advocated SDF as an antibacterial and caries preventive agent.
Another study conducted by Nishino and Massler in 197726 briefly discussed the caries score of SDF-treated teeth was distinctively less than 8% stannous fluoride or silver nitrate treated tooth.</td></tr><tr><td></td><td></td><td>b. To prevent recurrent caries</td><td>Even after restoring with the best restoration available. The tooth is often vulnerable to bacterial invasion through spaces between the cavity walls and restoration. Hence, the tooth is susceptible to recurrent caries. A slight modification in resistance form is inherent to inhibit such caries growth.27 Therefore, treating the tooth with SDF before restoration can be functional.</td><td>Shimizu and Kawagoe 1976(20) used SDF before restoring a primary tooth and, after 26 months, discovered no recurrent caries.</td></tr><tr><td></td><td></td><td>c. To prevent caries with minimally invasive treatments.</td><td>Treatment in young patients is always known to be strenuous. Especially moisture control is a vast huddle as well, and the sound of the drill sometimes triggers fear or can cause dental anxiety. Hence, SDF would help arrest the caries growth, and later, when the young patient is rational enough to accept the treatment, invasive caries removal would be followed by permanent restoration.</td><td>Yamaga et al.16,28 Japan is known to be a pioneer in proposing this minimally invasive treatment approach.
Hihara et al. (1994)29 in Japan, McDonald and Sheiham (1994)30 in London, Llodra et al. (2005)31 in Cuba, and Braga et al. (2009)10 in Brazil all agree with this approach in their studies.
Yee et al. (2009)19 in Nepal discovered that SDF could arrest cavitated and incipient decay.</td></tr><tr><td>2.</td><td>Inhibitive</td><td>a. To arrest caries in primary teeth</td><td>The preschool population categories are often associated with deciduous dentition and are susceptible to 'early childhood caries.' Restoration in primary dentition is always less popular due to their temporary life span. But they play a vital role in the growth of the jaw and, indirectly, the development of the face. Therefore, it is of utmost importance to conserve them. Acute conditions like 'rampant caries' are known for their unpredictable pattern of destruction. SDF is used as an alternative to traditional zinc oxide eugenol restoration.32</td><td>Nishino et al. (1969)33 & Moritani et al. (1970)34 discovered an arrested growth of caries in children under SDF therapy compared to the one without it.
Lo and Lin (2002)8 found that SDF successfully arrested dentinal caries in primary anterior teeth in preschool children at a community-based Caries Control Program.</td></tr><tr><td></td><td></td><td>b. To arrest root caries</td><td>The prevalence of root caries in the geriatric population is at its peak, and its incidence is directly proportional to an increase in age.</td><td>Tan et al. (2010)35 and Zang et al. (2013)36 concluded that SDF effectively arrests root surface caries when applied annually.</td></tr><tr><td>3.</td><td>Desensitizing</td><td>To prevent sensitivity</td><td>The composition of SDF has a unique capability of sealing off dental tubules, preventing dental hypersensitivity.</td><td>Gottlieb et al. 21 suggested with work that the mechanism behind dentinal hypersensitivity and arresting dental caries are common.
Three researchers, Hatsuyama et al. (1967),37 Murase et al. (1969) 38 and Kimura et al. 39 (1971), have discovered SDF as the most efficacious against erosion and abrasion type of non-caries lesions and desensitizing dentin to cold, heat and mechanical sensations.
They could prove that after four applications of SDF, they saw no further effect in desensitization.</td></tr><tr><td>4.</td><td>Anti-infective</td><td>In Root canal treatment</td><td>Silver nitrate, combined with ammonia, had been advocated since the early 19th century as a chemical that can sterilize the area, leaving no bacterial species. Similarly, this combination can be employed in treating infected root canals.</td><td>Hiraishi et al. (2010) 40 documented that 3.8% of SDF is used as root canal irrigant or interappointment medicament, which would serve as an antibiotic in nonaesthetic areas where darkening due to SDF is not a significant concern.
Okamoto et al. 41 discovered that the application of SDF governs the frequency of treatment.
Mathew et al. 2012 42 found that SDF, when used as an endodontic irrigation solution, has a beneficial effect in sterilizing root canals and circum-pulpal dentin.</td></tr><tr><td>5.</td><td>Miscellaneous</td><td>Community dental health program.</td><td>Funding a community health program by a federal or non-federal institution is often challenging. To overcome such financial burdens, SDF can be a replacement or an alternative to the expensive restorative materials and instrumentation used in it.</td><td>Bedi and Infirri (1999) 43 pointed out crucial benefits that prove SDF is expensive in controlling caries at a community level.</td></tr></table>
## VI. LIMITATIONS OF SILVER DIAMINE FLUORIDE
The major drawback of using SDF to arrest caries is that it imparts staining, usually black. For this reason, SDF is never preferred in the aesthetic zone. To overcome the black staining, applying potassium iodide after SDF application will cause a reaction between the free silver ions of SDF to form silver iodide, a white crystal. Knight et al. $^{12}$ were the pioneers in establishing this technique.
Another drawback SDF has can be related to the operator as well. SDF tends to stain skin, clothes, or anything that encounters it. Sometimes, these stains are permanent or stay for a long time. Moreover, SDF has a metallic taste, occasionally unpleasant for the patients. Furthermore, in surrounding structures in the oral cavity, SDF can cause gingival or mucosal irritation.
## VII. CONCLUSION
Silver Diamine Fluoride emerges as a promising agent in the contemporary armamentarium of dental care, showcasing its efficacy in caries arrest, indirect pulp capping, and dentin hypersensitivity management. While its aesthetic consequences pose a challenge, ongoing research endeavors and potential strategies, such as the post-treatment application of potassium iodide, indicate a commitment to refining its clinical application.
This review consolidates evidence from diverse studies worldwide, comprehensively evaluating SDF's clinical applications, limitations, and future perspectives. As dentistry progresses toward more patient-centered and minimally invasive approaches, Silver Diamine Fluoride stands as a beacon of innovation, contributing to the evolution of preventive and therapeutic strategies in the field.
Generating HTML Viewer...
References
43 Cites in Article
Shalin Shah,Vijay Bhaskar,Karthik Venkatraghavan,Prashant Choudhary,Ganesh M.,Krishna Trivedi (2014). Silver Diamine Fluoride: A Review and Current Applications.
M Rathee,A Sapra (2024). Proceedings of the 20th International Conference on Applied Computing 2023 and 22nd International Conference on WWW/Internet 2023, held in Madeira Island, Portugal from 21 to 23 October 2023.
G Nikiforuk (1985). It is understanding dental caries.
Burton Edelstein (1995). Policy issues in early childhood caries.
V Baelum,Van Palenstein,W Helderman,A Hugoson,R Yee,O Fejerskov (2007). A global perspective on changes in the burden of caries and periodontitis: implications for dentistry.
R Yamaga,M Nishino,S Yoshida,I Yokomizo (1972). Diamine silver fluoride and its clinical application.
Inshiya Alazhar Contractor,M Girish,M Indira (2021). Silver Diamine Fluoride: Extending the Spectrum of Preventive Dentistry, a Literature Review.
A Lansdown (2002). Silver. I: Its antibacterial properties and mechanism of action.
A Lansdown (2006). Silver in health care: antimicrobial effects and safety in use.
A Shimizu,M Kawagoe (1976). A clinical study of diamine silver fluoride on recurrent caries.
Gottlieb B (1947). Dental caries and related subjects.
K Selvig (1968). Ultrastructural changes in human dentine exposed to a weak acid.
T Suzuki,S Sobue,H Suginaka (1976). Mechanism of antiplaque action of diamine silver fluoride.
R Sato,Y Sailo (1970). Clinical Application of Silver Ammonia Fluoride (Saforide) to Children.
M Nishino,M Massler (1977). Immunization of caries-susceptible pits and fissures with a diamine silver fluoride solution.
John Manappallil (2015). Basic Dental Materials.
I Yanagida,M Nishino,T Hano (1971). Figure 1: The effects of fluoride, silver nitrate, and silver diamine fluoride on bacteria and teeth..
T Hihara,M Nishino,Y Yasutomi (1994). Effects of diamine silver fluoride on arrestment and prevention of caries in primary tooth.
S Mcdonald,A Sheiham (1994). A clinical comparison of non-traumatic methods of treating dental caries.
T Roberson,H Heymann,E Swift,C Sturdevant (2006). Sturdevant's Art and Science of Operative Dentistry.
Suchitra Nelson,Jeffrey Albert,Peter Milgrom (2020). Comparative Effectiveness of Two Nonsurgical Treatments to Reduce Oral Health Disparities From Untreated Tooth Decay in Older Adults: Protocol for a Cluster Randomized Trial.
C Chu,E Lo,H Lin (2002). Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children.
R Yee,C Holmgren,J Mulder,D Lama,D Walker,W Van Palenstein Helderman (2009). Efficacy of silver diamine fluoride for Arresting Caries Treatment.
M Braga,F Mendes,M De Benedetto,J Imparato (2009). Effect of silver diamine fluoride on incipient caries lesions in erupting permanent first molars: a pilot study.
G Knight,J Mcintyre,G Craig,Mulyani,P Zilm,N Gully (2007). Differences between normal and demineralized dentine pretreated with silver fluoride and potassium iodide after an <i>in vitro</i> challenge by <i>Streptococcus mutans</i>.
G Knight,J Mcintyre,G Craig,Mulyani,P Zilm,N Gully (2007). Differences between normal and demineralized dentine pretreated with silver fluoride and potassium iodide after an <i>in vitro</i> challenge by <i>Streptococcus mutans</i>.
A Russell,W Hugo (1994). 7 Antimicrobial Activity and Action of Silver.
R Yamaga,M Nishino,S Yoshida,I Yokomizo (1972). Diamine silver fluoride and its clinical application.
F Zheng,I Yan,D Duangthip,S Gao,E Lo,C Chu,; Llodra,T Ramos,M Morato (2005). Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36month clinical trial.
Von Naegeli,V (1893). Unknown Title.
M Nishino,S Yoshida,S Sobue,J Kato,M Nishida (1969). TOPICALLY APPLIED SODIUM FLUORIDE AND DENTAL CARIES.
Y Moritani,M Doi,K Yao (1970). Clinical evaluation of silver diamine fluoride (Saforide) in controlling caries of deciduous teeth.
H Tan,E Lo,J Dyson,Y Luo,E Corbet (2010). A randomized trial on root caries prevention in elders.
W Zhang,C Mcgrath,E Lo,J Li (2013). Silver diamine fluoride and education to prevent caries among community-dwelling elders.
M Hatsuyama,T Toda,I Sckine (1967). Effect of Silver Ammonia Fluoride on Hypersensitive Dentin.
M Murnse,H Takai (1969). Silver Diamine Fluoride to Relieve Older Adults’ Dentin Hypersensitivity.
K Kimura,Y Iso,M Ohno (1971). Clinical Test of Diamine Silver Fluoride (Saforide) Applied to Hypersensitive Dentin.
N Hiraishi,C Yiu,N King,J Tagami,F Tay (2010). Antimicrobial efficacy of 3.8% silver diamine fluoride and its effect on root dentin.
E Okamoto,H Kutsuna,Y Nakamura (1971). Effect of Diamine Silver Fluoride on Treatment of Infected Root Canal Part 1: On the Number of Treatments Required for Root Canal Filling.
Vinod Mathew,Koppolu Madhusudhana,Nuvulla Sivakumar,Thangala Venugopal,Redderu Reddy (2012). Anti-microbial efficiency of silver diamine fluoride as an endodontic medicament – An ex vivo study.
R Yee,C Holmgren,J Mulder,D Lama,D Walker,W Van Palenstein Helderman (2009). Efficacy of Silver Diamine Fluoride for Arresting Caries Treatment.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Dr. Shivam Patel. 2026. \u201cSilver Diamine Fluoride In Dentistry: A Review Of Clinical Applications And Future Prospects\u201d. Global Journal of Medical Research - J: Dentistry & Otolaryngology GJMR-J Volume 24 (GJMR Volume 24 Issue J1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































