Obstructive sleep apnea syndrome (OSAS) is a respiratory illness that is associated with recurrent episodes of either partial or full obstruction of the upper airways, or apnea, among other sleep disorders. This study aims to analyze, through a literature review, whether orthodontic treatment can be a good treatment strategy for this type of disorder. We performed a database search on Scopus, Web of Science, and Pubmed with the keywords OSA(S) and orthodontics to select the papers under evaluation. The criteria for inclusion were articles related to OSA(S) children undergoing an orthodontic treatment and clinical studies or case series, excluding systematic reviews, narrative reviews, meta-analyses, adult studies, animal models, and in vitro studies.
## I. INTRODUCTION
Sleep is a periodic, natural, biological occurrence that includes the loss of awareness, a reduction in or partial cessation of nerve center functioning, and a slowdown in the performance of certain bodily activities like breathing, circulation, and metabolism [1].
It turns out that sleep is essential to human existence; just consider that each person sleeps for roughly one-third of their lifetime [2,3]. Because it is intimately linked to the preservation of brain metabolism, the health of the rest of the cardiovascular system, and the equilibrium of glucose metabolism, it plays a significant role in preserving psychophysical balance [4-12]. Therefore, it is easy to see how sleep abnormalities could impact a person's psychological and mental health [13-15]. Speaking of a child makes the situation considerably more significant [16-18]. Consider that a newborn's first few months of life are spent sleeping for $70 - 80\%$ of the day [19]. The first week of life is estimated to require $16 - 17\mathrm{h}$ of sleep, followed by $15\mathrm{h}$ at around 6 months, $14\mathrm{h}$ at roughly 1 year, $13\mathrm{h}$ at around 2 years, and $12\mathrm{h}$ at around 3 years [20]. After the age of six, children typically sleep for nine hours, ten hours, and eight hours during puberty [21-32]. The young sleep more because sleep serves multiple purposes, including boosting immune system strength, allowing the brain to "cleansse" waste toxins produced during wakefulness, consolidating memory and learning, promoting the release of growth hormones, and promoting brain development (especially REM sleep) [19,33,34]. Because of this, it is important to try to catch sleep disturbances in children early, on as they have a significant impact on their health. Obstructive sleep apnea syndrome (OSAS) is a respiratory illness that is associated with recurrent episodes of either the partial or full obstruction of the upper airways, or apnea, among other sleep disorders [35-37]. They can be of two types: peripheral, caused by a mechanical obstruction of the airways, or central, caused by a disruption in the neurological system's capacity to stimulate the breathing muscles [38,39]. Just consider how common this is: depending on the case studies and polysomnographic criteria employed, the frequency of obstructive sleep apnea syndrome (OSAS) in children ranges from $0.69\%$ to $5.7\%$ [40,41].
### a) Risk Factors
The main risk factors for the development of OSAS in children are adenotonsillar hypertrophy, obesity, craniofacial abnormalities, neuromuscular disorders, and hypercapnia \[42\](Table 1).
Table 1: Some Pathologies in Which OSAS May be Present [4]
<table><tr><td>Diseases with a Craniofacial Component</td><td>Associations with Soft Tissues</td><td>Neuromuscular Associations</td><td>Inflammatory Associations</td></tr><tr><td>Apert's syndrome</td><td>Obesity</td><td>Cerebral palsy</td><td>Asthma</td></tr><tr><td>Crouzon's syndrome</td><td>Cystic hygroma</td><td>Hypothyroidism</td><td>Metabolic syndrome</td></tr><tr><td>Pfeiffer's syndrome</td><td>Papillomatosis (oroparingea)</td><td>Achondroplasia</td><td>Sickle cell disease</td></tr><tr><td>Pierre-Robin syndrome</td><td>Prader-Willi syndrome</td><td>Patients with cleft palate after repair</td><td></td></tr><tr><td>Treacher Collins syndrome</td><td>Mucopolysaccharidosis</td><td>Down syndrome</td><td></td></tr><tr><td>Goldenhar syndrome (hemifacial microsomy)</td><td>Beckwith-Wiedernann's syndrome</td><td></td><td></td></tr><tr><td>Atresia/coanal stenosis</td><td>Down syndrome</td><td></td><td></td></tr><tr><td>Hallermann-Streiff's syndrome</td><td>Syndromes with cleft</td><td></td><td></td></tr><tr><td>Klippel-Feil syndrome</td><td></td><td></td><td></td></tr><tr><td>Osteopetrosis</td><td></td><td></td><td></td></tr><tr><td>Sickle cell anemia (sickle cell disease)</td><td></td><td></td><td></td></tr><tr><td>Syndromes with cleft</td><td></td><td></td><td></td></tr></table>
## i. Hypertrophy of Adenotozillary
The most typical risk factor for the onset of OSAS is adenotonsillary hypertrophy. Adenotonsillary hypertrophy in children peaks in occurrence between the ages of 2 and 6 [43-45]. Within the same age range, the transverse section and volume of the upper airways are smaller, and the adenotonsillary volume-to-airway ratio is favorable to the former [46-48]. After six years, the ratio reverses, and the airway's transverse volume/section increases, but this is typically not accompanied by an increase in tonsillar or adenoid volume (the latter often tends to decline until normalization is achieved) [11,49-51]. Significant obstruction of the upper respiratory tract can occur when the tonsils and adenoids increase their encumbrance in the coan space and the hypopharynx, respectively [52-54]. However, significant adenotonsillary hypertrophy must still be linked to an upper airway-relative hypotonia for OSAS to manifest [55,56]. There is no obvious correlation between the adenoids and tonsils' sizes and the severity of OSAS, and not all children with notable adenotonsillary hypertrophy have OSAS [57-59].
The condition of mono- or bilateral cleft lip and palate also affects the volume of the airway and nasopharyngeal space. A study by Kiaee showed a significant reduction in oropharyngeal and total volume in 30 patients aged 9 to 12 years with unilateral cleft lip and palate compared with 30 age- and sex-matched controls $(p < 0.05)$ [60].
## ii. Obesity
Owing to the substantial quantities of adipose tissue that are accumulated at the level of the ribs, upper airways, and abdomen, obesity results in a reduction in minute ventilation, as well as static and dynamic lung volumes and capacities [61,62]. The close relationship between respiratory disorders in sleep and obesity and, specifically, between OSAS and obesity can be explained by the combination of changes in respiratory function brought on by obesity and those physiologically determined by sleep [61]. OSAS is far more common in obese subjects than in the general population [63-66]. Prevalence values range from $14\%$ to $78\%$ [67]. These differences result from how obesity and OSAS are defined by different authors [68-73]. Studies have shown that the degree of obesity and the severity of OSAS are correlated and that adenotonsillary hypertrophy is more common as a risk factor in obese subjects than in the non-obese population with OSAS [18,74,75].
## iii. Craniofacial Syndromes
The obstruction and appearance of OSAS are linked to primitive skeletal anatomical modifications of the upper airways, which are connected to syndromes of the craniofacial region [76,77]. Anatomical abnormalities in the upper airways associated with hypotonia and, in some cases, obesity may account for the unique prevalence of OSAS in this population [78-81]. A typical example of this would be the clinical picture of Down syndrome.
## iv. Neuromuscular Diseases
OSAS is more common in children with neuromuscular diseases because of muscle hypotonia, which is frequently brought on by scoliosis, restrictive dysventilatoria syndrome, and muscle pump deficiency. These children exhibit dysventilatorial or atelectasic areas more frequently because of their lack of cough and relative incapacity to clear respiratory secretions. These variables favor the appearance of changes in gas exchanges by changing the ventilation/perfusion ratio.
## v. Hypercapnia
An elevated blood carbon dioxide level is among the signs and symptoms associated with hypercapnia.
Abnormalities in the heart or lungs, such as respiratory acidosis or altered acid-base balance, are often the cause of this phenomenon. The inadequate ventilation of the alveoli is another common cause. Children are generally more likely than adults to suffer from hypercapnia when they sleep.
## vi. Pediatric OSAS Symptoms and Signs
The most common symptoms of OSAS include chronic and persistent snoring (HS), often with breathing pauses, paradoxical or otherwise difficult night breathing, sleeping disorders with frequent night awakenings, excessive night sweating, and occasionally secondary enuresis (in a child who has acquired urinary continence for at least 6 months). Additional indications and symptoms at night include nightmares, agitation, adopting specific sleeping positions (such as saluting Mohammed), and a posture that causes the neck to extend excessively. Children with OSAS may exhibit signs and symptoms during the day, including excessive daytime sleepiness, headaches upon waking, irritability, and poor academic performance. There are occasionally opposing expressions in the two more traditional phenotypes. The adenotonsillar phenotype is often characterized by thinness and inadequate growth in addition to facies adenoidea. The issue in the obese phenotype is the opposite and is typified by overgrowth (Table 2).
Table 2: Symptoms and Signs of Pediatric OSAS [3]
<table><tr><td>Night Symptoms</td><td>Daytime Speaker</td><td>Signs</td></tr><tr><td>Snoring</td><td>Difficulty awakening</td><td>Tonsil hypertrophy</td></tr><tr><td>Gaspung</td><td>Lack of rest upon waking</td><td>High/wide lingual position</td></tr><tr><td>Noisy breathing (typically inspiratory)</td><td>Drowsiness</td><td>Growth disorders (obesity, insufficient growth)</td></tr><tr><td>Respiration paradox</td><td>Hyperactivity</td><td>Pulmonary hypertension</td></tr><tr><td>Indentations (jugular or rib)</td><td>Aggression, bad mood</td><td>Systemic hypertension</td></tr><tr><td>Apnee testifies</td><td>Oral respiration</td><td>Craniofacial abnormalities</td></tr><tr><td>Restless sleep</td><td>Meager appetite</td><td>Laryngeal</td></tr><tr><td>Hyperextension of the neck</td><td>Dysphagia</td><td>Obstruction of the nasal airways</td></tr><tr><td>Oral respiration</td><td>School difficulties</td><td>Hypotonia</td></tr><tr><td>Night sweating</td><td>Daytime speaker</td><td>Gastroesophageal reflux</td></tr></table>
### b) Complications
There are three methods by which OSAS complications are assessed:
Arousals, or micro-awakenings, at the conclusion of hypnotic episodes; sporadic hypoxias with fast re-oxygenation (following the outlet at the end of apneic episodes), linked or unrelated to hypercapnia; and changes in intrathoracic pressure during obstructive events caused by respiratory effort.
These three processes function by initiating an intricate web of oxidative stress, free radical and pro inflammatory cytokine release, elevated phlogosis indexes, epithelial dysfunction, and sympathetic nervous system activation. The result is decreased vagal tone; catecholamine release; and elevated heart rate and variability. Neurocognitive and behavioral issues, growth retardation, systemic arterial hypertension, pulmonary hypertension, and disorders of the cardiovascular and metabolic systems are all encouraged by this intricate network (Table 3).
Table 3: Complications of OSAS [2]
<table><tr><td>Metabolic</td><td>Neurocognitive</td><td>Cardiovascular</td></tr><tr><td>Increased C-reactive protein</td><td>Decreased quality of life</td><td>Autonomic dysfunction</td></tr><tr><td>Insulin resistance</td><td>Aggressive behavior</td><td>Systemic hypertension</td></tr><tr><td>Hypercholesterolemia</td><td>Poor school performance</td><td>Absence of drop in blood pressure in sleep</td></tr><tr><td>Increased transaminases</td><td>Depression</td><td>Left ventricular dysfunction</td></tr><tr><td>Reduced insulin-like growth factor</td><td>Attention deficit</td><td>Pulmonary hypertension</td></tr><tr><td>Reduced/altered growth hormone secretion</td><td>Hyperactivity</td><td>Variability of heart rate altered</td></tr><tr><td></td><td>Moodiness</td><td>Increased vascular endothelial growth factor</td></tr></table>
### c) Management
## i. Adenotonsillectomy (AT)
With an estimated $70 - 100\%$ case efficacy, adenotonsillary hypertrophy is still the most frequent cause of OSAS in children, and the suggested course of treatment is still AT. A polysomnographic check will be scheduled following AT to determine whether any OSAS is still present.
## ii. CPAP
Nasal continuous positive airway pressure, or CPAP, is a successful treatment for OSAS even in younger children. However, a major barrier to the efficient use of CPAP can be treatment adherence. Because of this, when AT is a more sensible option, it is not recommended to use CPAP as the first line of treatment for OSAS. However, CPAP is recommended for children who do not react well to surgery, children for whom surgery is not recommended, and children whose families refuse to give their consent for surgery.
## iii. Medical Therapy
Numerous investigations have evaluated the effectiveness of leukotriene antagonists, such as montelukast, and topical nasal corticosteroids, such as fluticasone and budesonide, in the treatment of pediatric OSAS. Topical nasal corticosteroids are helpful for mild OSAS, but they should not be the only treatment for moderate or severe OSAS.
## iv. Bariatric Surgery
In 2012, guidelines were released regarding the use of bariatric surgery to treat severe obesity in carefully selected adolescents. Numerous studies have demonstrated how well gastric bandages, gastric bypasses, and gastrectomy sleeves work to lower apnea indices (AHIs) and body mass indices (BMIs).
## v. Orthodontic Treatment
RME, or rapid maxillary expansion, has been used as a treatment for pediatric OSAS. The goal of this orthodontic procedure is to increase the hard palate's transverse diameter by reopening the mid-palatal suture. This is accomplished by using a stationary apparatus with an expansion screw for approximately three to four months. Children with maxillary contraction and dental malocclusion typically undergo such a procedure.
## II. MATERIALS AND METHODS
### a) Protocol and Registration
This systematic review was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA), and it was submitted to PROSPERO with number ID 490431.
### b) Search Processing
We performed a search of databases such as Scopus, Web of Science (WoS), and PubMed using the keywords "OSA(S)" and "orthodontics" to select papers suitable for this topic, and the search was related to the last ten years (December 2013–December 2023).
### c) Eligibility Criteria
The reviewers, in a double-blind manner, included papers that satisfied the following criteria for inclusion: (1) articles related to OSA(S) children undergoing an orthodontic treatment; (2) clinical studies or case series.
Exclusion criteria were represented by reviews (systematic and/or narrative) with/without meta-analyses, studies regarding adult populations, animal models, and in vitro studies.
### d) Data Processing
The screening procedure, carried out by reading the article titles and abstracts chosen in the earlier identification step, allowed for the exclusion of any publications that varied from the themes looked at, and the full texts of publications previously included were then read. The reviewers discussed the selected articles, and in cases of disagreement, a third reviewer (FI) was consulted.
### e) Quality Assessment
The quality of the included papers was assessed by two reviewers, R.F. and E.I., using ROBINS, a tool developed to assess the risk of bias in the results of non-randomized studies that compare the health effects of two or more interventions. Seven points were evaluated, and each was assigned a degree of bias. A third reviewer (F.I.) was consulted in the event of a disagreement until an agreement was reached.
## III. RESULTS
Keyword searches of the Web of Science (40), Scopus (11), and PubMed (705) databases yielded a total of 756 articles.
The subsequent elimination of duplicates (42) resulted in the inclusion of 714 articles.
Of these 714 studies, 665 were excluded because they deviated from the previously defined inclusion criteria (383 off-topic, 2 vitro/animal studies, 122 reviews, 135 adult studies, 23 no free full-text).
The screening phase ended with the selection of 16 publications for this work.
The PRISMA flowchart of this review is summarized in Figure 1, and the data from each selected study (author(s), type of study, aim of the study, materials, and results) are reported in Table 4.
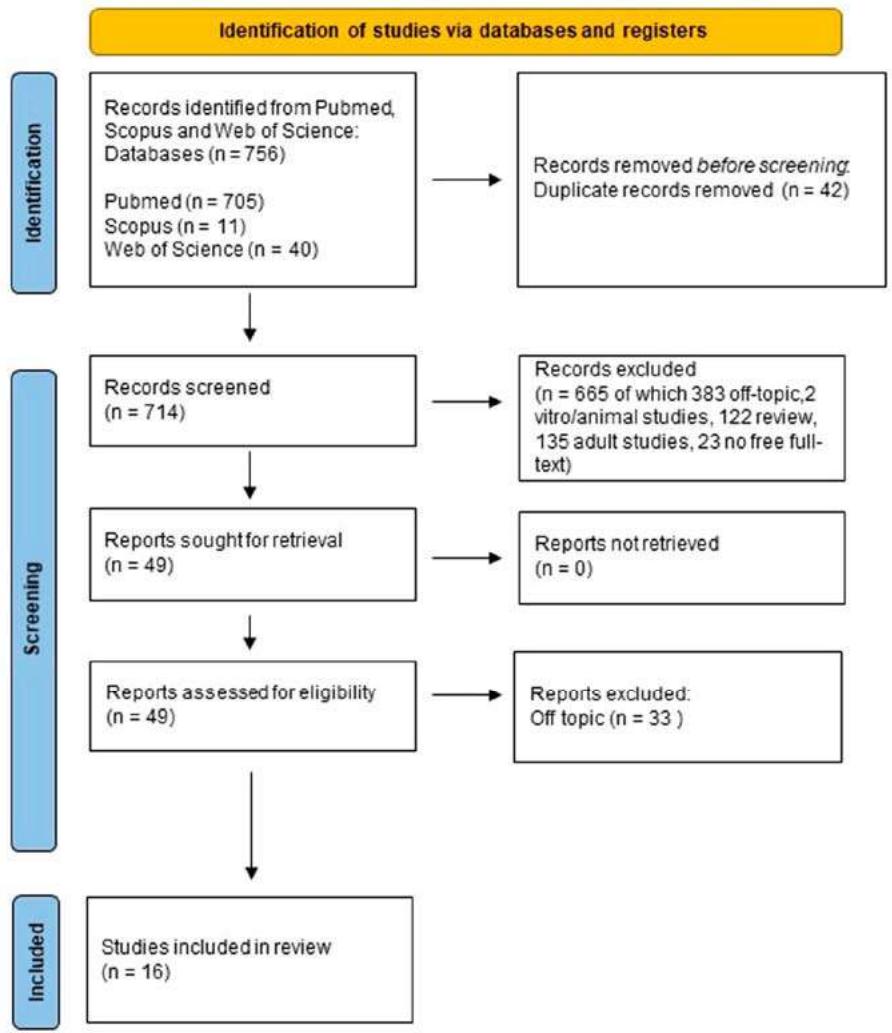 Figure 1: PRISMA Flowchart used in this Review Paper
Quality Assessment and Risk of Bias
The risk of bias in the included studies is reported in Scheme 1. Regarding bias due to confounding, most studies have a high risk. The bias arising from measurement is a parameter with a low risk of bias. The majority of studies have a low risk of bias because of bias in the selection of participants. Bias due to post-exposure cannot be calculated because of high heterogeneity. Bias due to missing data is low in the majority of studies. Bias arising from the measurement of the outcome is low. Bias in the selection of the reported results is high in the majority of studies. The final results show that four studies have a low risk of bias, six studies have a high risk of bias, three have a very high risk of bias, and the remainder have a questionable risk of bias.
Table 4: Examined Articles
<table><tr><td>Authors (Year)</td><td>Type of Study</td><td>Aim of the Study</td><td>Materials</td><td>Results</td></tr><tr><td>Caruso et al., 2023 [82]</td><td>Clinical study</td><td>To evaluate the cephalometric variations in upper airway dimensions and OSA-related clinical conditions after orthodontic treatment with an RME and the Delaire mask in patients affected by class III malocclusion.</td><td>In total, 14 children, ages 6 to 10, with m</td><td></td></tr><tr><td>Keerthana et al., 2022 [92]</td><td>Case series</td><td>To summarize the results of using the AdvanSync2 Class II corrector in the treatment of three orthodontic patients who complained of breathi</td><td></td><td></td></tr><tr><td>Machado-Júnior et al., 2016 [93]</td><td>Pilot study</td><td>To assess mandibular advancement appliance in children who have OSA. Adolescents diagnosed as apneic were those with an apnea-hypopnea</td><td></td><td></td></tr><tr><td>Medina et al., 2022 [94]</td><td>Clinical study</td><td>To ascertain if using this equipment causes healthy children's upper airways to enlarge and their sleep-breathing habits to improve.</td><td>In total, 39 healthy children: 20 for the activator group; 19 for the control group.</td><td>By opening the upper airw</td></tr><tr><td>Zhao et al., 2015 [96]</td><td>Pilot Study</td><td>To find out if class II hyperdivergent individuals undergoing complete orthodontic treatment are affected differently by the existence of OSA.</td><td></td><td>Pa</td></tr><tr><td>Zreaqat et al., 2023 [97]</td><td>CBCT study</td><td>To assess rapid maxillary expansion (RME)'s long-term effectiveness in treating a group of children with obstructive sleep apnea (OSA).</td><td></td><td>In</td></tr></table>

Scheme 1: Bias Assessment [82-97]
<table><tr><td rowspan="2"></td><td colspan="8">Risk of bias domains</td></tr><tr><td>D1</td><td>D2</td><td>D3</td><td>D4</td><td>D5</td><td>D6</td><td>D7</td><td>Overall</td></tr><tr><td>Caruso et al. 2023</td><td>-</td><td>+</td><td>+</td><td>-</td><td>+</td><td>-</td><td>-</td><td>-</td></tr><tr><td>Yoon et al. 2022</td><td>-</td><td>-</td><td>-</td><td>+</td><td>-</td><td>-</td><td>+</td><td>-</td></tr><tr><td>Pirelli et al. 2015</td><td>-</td><td>!</td><td>!</td><td>X</td><td>-</td><td>-</td><td>X</td><td>!</td></tr><tr><td>Villa et al. 2015</td><td>-</td><td>-</td><td>+</td><td>+</td><td>-</td><td>-</td><td>+</td><td>-</td></tr><tr><td>Pirelli et al. 2019</td><td>?</td><td>-</td><td>+</td><td>!</td><td>+</td><td>+</td><td>X</td><td>!</td></tr><tr><td>Pirelli et al. 2021</td><td>X</td><td>+</td><td>+</td><td>X</td><td>-</td><td>+</td><td>X</td><td>X</td></tr><tr><td>Kim et al. 2022</td><td>-</td><td>X</td><td>+</td><td>-</td><td>-</td><td>-</td><td>-</td><td>X</td></tr><tr><td>Li et al. 2022</td><td>-</td><td>+</td><td>X</td><td>X</td><td>+</td><td>-</td><td>+</td><td>X</td></tr><tr><td>Chuang et al. 2019</td><td>X</td><td>-</td><td>+</td><td>X</td><td>+</td><td>+</td><td>-</td><td>X</td></tr><tr><td>Ghodke et al. 2014</td><td>X</td><td>+</td><td>-</td><td>-</td><td>-</td><td>+</td><td>-</td><td>X</td></tr><tr><td>Keerthana et al.</td><td>X</td><td>+</td><td>+</td><td>-</td><td>+</td><td>X</td><td>+</td><td>+</td></tr><tr><td>Machado-Júnior et al. 2016</td><td>-</td><td>+</td><td>X</td><td>+</td><td>-</td><td>X</td><td>+</td><td>+</td></tr><tr><td>Medina et al. 2022</td><td>X</td><td>+</td><td>X</td><td>-</td><td>+</td><td>X</td><td>+</td><td>+</td></tr><tr><td>Zhang et al. 2013</td><td>X</td><td>+</td><td>X</td><td>+</td><td>+</td><td>X</td><td>+</td><td>+</td></tr><tr><td>Zhao et al. 2015</td><td>?</td><td>-</td><td>+</td><td>!</td><td>+</td><td>+</td><td>X</td><td>!</td></tr><tr><td>Zreaqat et al. 2023</td><td>X</td><td>+</td><td>+</td><td>X</td><td>-</td><td>+</td><td>X</td><td>X</td></tr></table>
## IV. DISCUSSION
### a) OSAS Treatment with Rapid Palatal Expander
## i. Effectiveness of RPE in Modifying the Upper Airway
A 2023 clinical study by Caruso et al. evaluated cephalometric changes recorded in 14 young patients affected by class III malocclusion and OSAS treated with RPE and Delaire's mask. In the cephalometric analysis, carried out on pre- and post-treatment laterolateral radiographs, in addition to the classic values for verticality and sagittality, millimeter measurements of upper airway space dimensions were examined. At the end of therapy, there was a statistically significant increase in linear upper airway measurements and oropharyngeal and nasopharyngeal dimensions in all patients, creating an improvement in airway patency and OSAS-related clinical conditions [82].
A 2016 retrospective study by Yoon et al. evaluated the effectiveness of REP in decreasing palatine tonsil and adenoid volume in pediatric patients with OSA. Sixty children with an average age of 8 years were split into a study group treated with REP and a control group that received no treatment. At the end of therapy, patients treated with REP showed a statistically significant reduction in the volume of tonsils and adenoids in contrast to patients in the control group, in whom there was no improvement. This work is very interesting because it represents the first clinical study to quantify changes in tonsil volume following palatal expansion [83].
Kim et al., in a 2022 clinical study, assessed changes in respiratory function related to increased upper airway volume in patients with OSA treated with RPE. In all 26 cases treated, there was an increase in the size of the nasomaxillary complex, with improvement in parameters related to OSA: there was a reduction in AHI and oxygen saturation values, and snoring had markedly improved \[88\](Figure 2).
 Figure 2: RPE Device
## ii. Radiographic Evaluation of the Effects of RPE
Pirelli et al., in a 2019 clinical study, evaluated the skeletal effects of RPE therapy in children with OSA through low-dose computed tomography (CT) measurements of the first molar angulation, maxillary base width, nasal cavity width, and the mid-palatal suture opening. The examinations performed demonstrated effective mid-palatal suture opening in all treated cases and improvements in the other parameters considered [86]. The same group of authors, in a 2021 study, demonstrated that RPE treatment is effective in children who have OSA and persistent snoring, causing an increase in the volume of the nasal cavity and nasopharynx. An increase in maxillary size results in an increase in upper airway volume, improving nasal breathing. The findings demonstrate that RPE therapy can eliminate obstructive sleep-breathing disorders and restore and enhance normal nasal airflow. The 19 children included in the study underwent CBCT before and after RPE treatment, and orthodontic and otolaryngological examination to confirm the above results [87].
## iii. Alternative Treatments in Cases of RPE Failure
A 2022 clinical study by Li et al. investigated the effects of skeletally fixed transpalatal distraction (TPD) on nasomaxillary expansion in patients with OSA previously treated with RPE. These patients, although they had resolved their malocclusions, still had residual OSA. As a result of this additional treatment, apnea episodes were significantly reduced: a nearly parallel anteroposterior opening of the mid-palatal suture enables the enlargement of the entire nasal passage with improved airflow characteristics in the nasal and pharyngeal airways. Improved airflow characteristics significantly correlated with enhanced polysomnographic results, indicating that nasomaxillary expansion is a feasible therapeutic option for patients who have previously undergone expansion [89].
## iv. Long-Term Effectiveness
A 2015 clinical study by Pirelli et al. followed a group of 31 pediatric patients diagnosed with OSA treated with RPE over time. The patients, at the start of treatment, presented maxillary contraction in the absence of tonsillar and adenoid hypertrophy. At the end of treatment, annual follow-up was performed for the next 12 years. A total of 23 individuals completed follow-up and underwent final PSG. All patients showed stable orthodontic outcomes and resolution of OSA. RPE treatment, therefore, was also shown to be effective in the long term [84].
The same conclusions were reached in a 2015 retrospective clinical study by Villa et al., in which the benefits of RPE therapy in the resolution of malocclusions characterized by a high and narrow palate in patients with OSA and moderate tonsillar hypertrophy were evaluated. At the 10-year follow-up, most patients had resolved their OSA issues, and the best results were seen in those who underwent an orthodontic treatment earlier [85].
### b) OSAS Treatment with Mandibular Advancement Devices
The condition known as obstructive sleep apnea (OSA) is characterized by the abnormal, intermittent total or partial blockage of breathing during sleep that interferes with regular ventilation. On the spectrum of obstructive breathing sleep disorders, it is the most severe kind [A]. Children with this kind of illness typically display symptoms throughout the day, such as irregularities in their behavior, development, cognitive abilities, and hearts [34].
Although the few data available now may imply that mandibular advancement appliances (MAAs) increase AHI scores, it is not possible to draw the conclusion that MAAs are useful in treating pediatric OSA. In 2016, in order to prove that evidence, Machado-Junior Almiro-José et al. conducted a randomized controlled pilot study.
They came to the conclusion that individuals who are hyperdivergent and undergoing thorough orthodontic treatment do not fare as well if they have OSA. Planning regular therapy for sleep-breathing problems and airway blockage should include an examination. The results of these children's orthodontic therapy may be influenced by early detection and the treatment of pediatric OSA [93].
One type of oral functional appliance used for the early treatment of children with mandibular retrognathia is called a twin block (TB) (Figure 3). Because of the mandible's forward location, TB could be an appropriate oral appliance for treating children with OSA [98].
In a preliminary study conducted in 2013, Chen Z. et al. aimed to determine the initial effectiveness and tolerability of TB treatment for children patients with mandibular retrognathia and OSAS [9,99-101]. Taking into account certain limitations in the study's design, such as the lack of a control group to compare with and the need to rule out other variables like growth that could have an impact on the findings, the authors came to the conclusion that TB appliances might help the selected patients with their facial profiles and OSA symptoms [95].
Ghodke S. et al., in a study conducted in 2014, analyzed the impact of TB appliance on the anatomy of pharyngeal airway passage (PAP) in a group of class II malocclusion patients in an age range of 8 to 14 years. They stated that, for class II malocclusion subjects, the TB appliance to treat mandibular retrusion enhanced PAP dimensions while maintaining the same pretreatment posterior pharyngeal wall thickness. Consequentially, by removing predisposing factors and adaptive alterations in the upper airway during infancy, class II correction using a TB device may help lower the likelihood of developing OSA as an adult [91].
 Figure 3: Twin Block Device
In a pilot study in 2018, Zhao T. et al. aimed to find out if OSA affects the orthodontic treatment outcome for class II hyperdivergent patients undergoing complete orthodontic therapy.
They highlighted how, in the young OSA patients selected for the study, the pattern of bone growth became more vertical, in contrast with the non-OSA group, where the pattern of bone growth became more horizontal. Along with that, both groups' treatment outcomes in terms of occlusion and sagittal bone growth were comparable [96].
Keerthana P. et al., in 2022, presented a case series to highlight the effectiveness of an AdvanSync2 Class II corrector in the treatment of three orthodontic patients with OSA conditions. The modifications to airway size after the use of AdvanSync2 were evaluated by comparing lateral cephalograms taken before and after therapy. In all three cases, a notable improvement in airway dimensions was seen [92].
In a 2019 comparative cohort research, Chuang Li-Chuan et al. assessed the quality of life and craniofacial and airway morphology in children with OSA before and after a year of passive myofunctional therapy (PMFT). The PMFT device tested consistently in a custom-designed oral appliance with a built-in tongue bead. For the duration of the study (1 year) every night while they slept, study participants were to wear their appliances and roll the bead with their tongues.
They came to the conclusion that PMFT can enhance nasal breathing during sleep, as well as mandibular growth and upper airway morphology in the oropharyngeal region. The OSA-18 survey indicated a significant improvement in the quality of life of treated patients, particularly in relation to emotional distress [90].
In a 2023 study, Zreaqat M. et al. used cone beam computed tomography (CBCT) in conjunction with three-dimensional analysis to evaluate the effects of TB appliance therapy on upper airway parameters and dimensions, as well as the apnea-hypopnea indexes (AHIs), in children with OSA who had class II malocclusions and mandibular retrognathia before and after completing myofunctional TB therapy.
It has been demonstrated that CBCT imaging is a reliable and accurate diagnostic method for examining craniofacial tissues and upper airways [97].
The authors segmented the upper airway into three regions (nasopharynx, oropharynx, hypopharynx), and for each region, they measured the airway volume and the minimum cross-sectional area (MCA) in the axial view.
They concluded that the TB therapy performed to treat class II mandibular retrognathic skeletal malocclusion led to a significant decrease in AHI but no change in nasopharynx parameters. Upper airway volume; the MCA; the anteroposterior and lateral distances of the MCA at the level of the oropharynx; the MCA at the level of the hypopharynx; and upper airway length were significantly increased as a result of the findings [97].
Since, as we have shown, different studies agree that the mandible forward advancement with an orthodontic activator can improve the AHI in pediatric patients who have both abnormal maxilla-mandible relationships and OSA, Medina C.C. et al., in 2022, were interested in verifying the theory that, in addition to its intended function of inducing mandibular development, activators may enhance the dimensions of skeletal class II children's upper airways to promote healthy sleep-breathing patterns even in the absence of sleep disturbances.
Many assessments, such as radiographic examinations of the upper airway, sleepbreathing monitoring, and questionnaires sent to parents and examined children, were used to test this theory.
They came to the conclusion that the activator not only allows for harmonic occlusion and healthy mandibular development but also widens the upper airway and lowers the frequency of disordered breathing events in children receiving this therapy, which enhances the quality of sleep and breathing [94].
## V. CONCLUSIONS
Respiratory sleep disorders are a rather common condition in the pediatric population, OSAS being the most common among them. As in other fields of science, intervention as early as possible can change the natural course of the disorder. In this regard, an early orthodontic intervention, such as REP or mandibular advancement with functional appliances, may be effective in the management of pediatric OSAS, suggesting that the correction of craniofacial structure imbalances during growth can reduce snoring and OSAS in children and young adolescents. Specifically, there is limited evidence to support mandibular advancement appliances (MAAs) in improving pediatric OSA, so further investigation is needed to establish their efficacy conclusively, while studies that have evaluated RPE in pediatric patients with obstructive sleep apnea syndrome (OSAS) have shown promising results, with significant cephalometric changes finding an increase in linear upper airway measurements and the subsequent expansion of nasal airflow. The goal of this early intercceptive treatment is clearly to restore the balance of the maxillary bone bases so that oral cavity functions (phonation, swallowing, breathing, and chewing) can be performed properly.
Further studies with a large number of patients are needed, especially on mandibular advancement devices used during the pediatric age, to evaluate their possible benefits in terms of OSAS-related symptoms and to develop structural modifications to improve airway morphology.
Author Contributions: Conceptualization, C.P., R.S., A.P., A.M. and G.D.; methodology, F.I., K.F. and G.L.; software, I.T. and A.P.; validation, R.S., G.D. and A.B.-F.; formal analysis, A.M.I., A.D.I., A.P., I.T. and C.P.; investigation, A.P., R.S., G.L., A.D.I. and A.M.I.; resources, C.P., A.B.-F. and A.P.; data curation, G.M., F.I., G.D., K.F., I.T. and G.L.; writing-original draft preparation, K.F., A.B.-F., A.M.I., I.T. and C.P.; writing-review and editing, G.M., R.S., I.T. and G.D.; visualization, A.M.I. and G.L.; supervision, G.M., A.D.I., A.P. and F.I.; project administration, F.I., G.D., K.F. and A.B.-F.; funding acquisition, A.M., K.F., A.B.-F. and F.I. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: Not applicable.
Informed Consent Statement: Not applicable.
Data Availability Statement: Not applicable.
Conflicts of Interest: The authors declare no conflicts of interest.
Generating HTML Viewer...
References
101 Cites in Article
C Marcus,L Brooks,K Draper,D Gozal,A Halbower,J Jones,M Schechter,S Ward,S Sheldon,R Shiffman (2012). Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome.
María Alonso-Álvarez,José Cordero-Guevara,Joaquin Terán-Santos,Mónica Gonzalez-Martinez,María Jurado-Luque,Jaime Corral-Peñafiel,Joaquin Duran-Cantolla,Leila Kheirandish-Gozal,David Gozal (2014). Obstructive Sleep Apnea in Obese Community-Dwelling Children: The NANOS Study.
L Reddy,P Madithati,B Narapureddy,S Ravula,S Vaddamanu,F Alhamoudi,G Minervini,S Chaturvedi (1920). Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study.
Shraddha Rathi,Saurabh Chaturvedi,Sabzar Abdullah,Geeta Rajput,Nasser Alqahtani,Mudita Chaturvedi,Vishwanath Gurumurthy,Ravinder Saini,Shashit Bavabeedu,Giuseppe Minervini (2023). Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention.
Noreen Qazi,Madhura Pawar,Preeti Padhly,Vivek Pawar,Cesare D’amico,Fabiana Nicita,Luca Fiorillo,Adela Alushi,Giuseppe Minervini,Aida Meto (2023). Teledentistry: Evaluation of Instagram posts related to bruxism.
Giuseppe Minervini,Rocco Franco,Maria Marrapodi,Vincenzo Ronsivalle,Ira Shapira,Marco Cicciù (2023). Prevalence of temporomandibular disorders in subjects affected by Parkinson disease: A systematic review and metanalysis.
Giuseppina Crescente,Giuseppe Minervini,Carmela Spagnuolo,Stefania Moccia (2022). Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain.
G Minervini,A Lucchese,L Perillo,R Serpico,G Minervini (2017). Unilateral Superior Condylar Neck Fracture with Dislocation in a Child Treated with an Acrylic Splint in the Upper Arch for Functional Repositioning of the Mandible.
M Kohler,S Thormaehlen,J Kennedy,Y Pamula,C Van Den Heuvel,K Lushington,A Martin (2009). Differences in the Association Between Obesity and Obstructive Sleep Apnea Among Children and Adolescents.
Melissa Xanthopoulos,Paul Gallagher,Robert Berkowitz,Jerilynn Radcliffe,Ruth Bradford,Carole Marcus (2015). Neurobehavioral Functioning in Adolescents With and Without Obesity and Obstructive Sleep Apnea.
Jeremy Hull,Roona Aniapravan,Elaine Chan,Michelle Chatwin,Julian Forton,Jayne Gallagher,Neil Gibson,Jill Gordon,Imelda Hughes,Renee Mcculloch,Robert Russell,Anita Simonds (2012). British Thoracic Society guideline for respiratory management of children with neuromuscular weakness.
D Gozal,Sleep (2009). Sleep Disorders and Inflammation in Children.
Linda Horwood,Robert Brouillette,Christine Mcgregor,John Manoukian,Evelyn Constantin (2014). Testing for Pediatric Obstructive Sleep Apnea When Health Care Resources Are Rationed.
Athanasios Kaditis,Leila Kheirandish-Gozal,David Gozal (2016). Pediatric OSAS: Oximetry can provide answers when polysomnography is not available.
G Nixon,A Kermack,G Davis,J Manoukian,K Brown,R Brouillette (2004). Planning Adenotonsillectomy in Children with Obstructive Sleep Apnea: The Role of Overnight Oximetry.
Vito Crincoli,Maria Anelli,Eleonora Quercia,Maria Piancino,Mariasevera Di Comite (2019). Temporomandibular Disorders and Oral Features in Early Rheumatoid Arthritis Patients: An Observational Study.
Hui-Leng Tan,David Gozal,Helena Ramirez,Hari Bandla,Leila Kheirandish-Gozal (2014). Overnight Polysomnography versus Respiratory Polygraphy in the Diagnosis of Pediatric Obstructive Sleep Apnea.
A Inchingolo,A Patano,M De Santis,G Del Vecchio,L Ferrante,R Morolla,C Pezzolla,R Sardano,L Dongiovanni,F Inchingolo (2023). Comparison of Different Types of Palatal Expanders: Scoping Review.
S Cantore,A Ballini,D Farronato,G Malcangi,G Dipalma,F Assandri,U Garagiola,F Inchingolo,D De Vito,N Cirulli (2016). Evaluation of an oral appliance in patients with mild to moderate obstructive sleep apnea syndrome intolerant to continuous positive airway pressure use: Preliminary results.
Alessio Inchingolo,Giuseppina Malcangi,Alexandra Semjonova,Angelo Inchingolo,Assunta Patano,Giovanni Coloccia,Sabino Ceci,Grazia Marinelli,Chiara Di Pede,Anna Ciocia,Antonio Mancini,Giulia Palmieri,Giuseppe Barile,Vito Settanni,Nicole De Leonardis,Biagio Rapone,Fabio Piras,Fabio Viapiano,Filippo Cardarelli,Ludovica Nucci,Ioana Bordea,Antonio Scarano,Felice Lorusso,Andrea Palermo,Stefania Costa,Gianluca Tartaglia,Alberto Corriero,Nicola Brienza,Daniela Di Venere,Francesco Inchingolo,Gianna Dipalma (2022). Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature.
Alessio Inchingolo,Assunta Patano,Giovanni Coloccia,Sabino Ceci,Angelo Inchingolo,Grazia Marinelli,Giuseppina Malcangi,Valentina Montenegro,Claudia Laudadio,Giulia Palmieri,Ioana Bordea,Emanuela Ponzi,Paola Orsini,Romina Ficarella,Antonio Scarano,Felice Lorusso,Gianna Dipalma,Massimo Corsalini,Mattia Gentile,Daniela Venere,Francesco Inchingolo (2021). Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report.
F Inchingolo,D Hazballa,A Inchingolo,G Malcangi,G Marinelli,A Mancini,M Maggiore,I Bordea,A Scarano,M Farronato (2022). Innovative Concepts and Recent Breakthrough for Engineered Graft and Constructs for Bone Regeneration: A Literature Systematic Review.
B Rapone,E Ferrara,L Santacroce,S Topi,A Gnoni,G Dipalma,A Mancini,M Di Domenico,G Tartaglia,A Scarano (2022). The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial.
D Dohan Ehrenfest,M Del Corso,F Inchingolo,G Sammartino,J.-B Charrier (2010). Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results.
Jakub Vanek,Jan Prasko,Samuel Genzor,Marie Ociskova,Krystof Kantor,Michaela Holubova,Milos Slepecky,Vlastimil Nesnidal,Antonin Kolek,Milan Sova (2020). Obstructive sleep apnea, depression and cognitive impairment.
A Inchingolo,S Ceci,A Patano,A Inchingolo,V Montenegro,C Di Pede,G Malcangi,G Marinelli,G Coloccia,M Garibaldi (2022). Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP ® Devices: A Retrospective Study.
Andrea Ballini,Gianna Dipalma,Ciro Isacco,Mariarosaria Boccellino,Marina Di Domenico,Luigi Santacroce,Kieu Nguyễn,Salvatore Scacco,Maura Calvani,Anna Boddi,Fabiana Corcioli,Lucio Quagliuolo,Stefania Cantore,Francesco Martelli,Francesco Inchingolo (2020). Oral Microbiota and Immune System Crosstalk: A Translational Research.
Giuseppe Minervini,Rocco Franco,Maria Marrapodi,Marco Di Blasio,Vincenzo Ronsivalle,Marco Cicciù (2023). Children oral health and parents education status: a cross sectional study.
M Alonso-Álvarez,J Terán-Santos,E Ordax Carbajo,J Cordero-Guevara,A Navazo-Egüia,L Kheirandish-Gozal,D Gozal (2015). Reliability of Home Respiratory Polygraphy for the Diagnosis of Sleep Apnea in Children.
J Carroll (2003). Obstructive Sleep-Disordered Breathing in Children: New Controversies, New Directions.
V Crincoli,A Ballini,L Fatone,M Di Bisceglie,G Nardi,F Grassi (2016). Risk Factors Associated with Coronavirus Disease 2019-Related Hospitalization in Rheumatoid Arthritis Patients.
R Goldoni,C Dolci,E Boccalari,F Inchingolo,A Paghi,L Strambini,D Galimberti,G Tartaglia (2022). Salivary Biomarkers of Neurodegenerative and Demyelinating Diseases and Biosensors for Their Detection.
C Isacco,A Ballini,D De Vito,K Nguyen,S Cantore,L Bottalico,L Quagliuolo,M Boccellino,M Di Domenico,L Santacroce (2021). Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders.
F Massa,S Gonsalez,A Laverty,C Wallis,R Lane (2002). The use of nasal continuous positive airway pressure to treat obstructive sleep apnoea.
Clete Kushida,Alejandro Chediak,Richard Berry,Lee Brown,David Gozal,Conrad Iber,Sairam Parthasarathy,Stuart Quan,James Rowley (2008). Clinical Guidelines for the Manual Titration of Positive Airway Pressure in Patients with Obstructive Sleep Apnea.
R Brouillette,J Manoukian,F Ducharme,K Oudjhane,L Earle,S Ladan,A Morielli (2001). Efficacy of Fluticasone Nasal Spray for Pediatric Obstructive Sleep Apnea.
Emmanouel Alexopoulos,Athanasios Kaditis,Efthimia Kalampouka,Eleni Kostadima,Nikiforos Angelopoulos,Vasiliki Mikraki,Nikolaos Skenteris,Konstantinos Gourgoulianis (2004). Nasal corticosteroids for children with snoring.
L Kheirandish-Gozal,D Gozal (2008). Intranasal Budesonide Treatment for Children with Mild Obstructive Sleep Apnea Syndrome.
Giuseppe Minervini,Rocco Franco,Maria Marrapodi,Luca Fiorillo,Gabriele Cervino,Marco Cicciù (2023). Economic inequalities and temporomandibular disorders: A systematic review with meta‐analysis.
A Inchingolo,S Ceci,G Coloccia,D Azzollini,G Malcangi,A Mancini,F Inchingolo,P Trerotoli,G Dipalma,A Patano (2023). Predictability and Effectiveness of Nuvola ® Aligners in Dentoalveolar Transverse Changes: A Retrospective Study.
Andrea Ballini,Stefania Cantore,Luca Signorini,Rajiv Saini,Salvatore Scacco,Antonio Gnoni,Alessio Inchingolo,Danila De Vito,Luigi Santacroce,Francesco Inchingolo,Gianna Dipalma (2021). Efficacy of Sea Salt-Based Mouthwash and Xylitol in Improving Oral Hygiene among Adolescent Population: A Pilot Study.
A Goldbart,J Goldman,M Veling,D Gozal (2005). Leukotriene Modifier Therapy for Mild Sleep-Disordered Breathing in Children.
Leila Kheirandish,Aviv Goldbart,David Gozal (2006). Intranasal Steroids and Oral Leukotriene Modifier Therapy in Residual Sleep-Disordered Breathing After Tonsillectomy and Adenoidectomy in Children.
M Farronato,D Farronato,A Giannì,F Inchingolo,L Nucci,G Tartaglia,C Maspero (2022). Effects on Muscular Activity after Surgically Assisted Rapid Palatal Expansion: A Prospective Observational Study.
G Minervini,C D'amico,M Cicciù,L Fiorillo (2023). Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches.
Giuseppe Minervini,Pierluigi Mariani,Luca Fiorillo,Gabriele Cervino,Marco Cicciù,Luigi Laino (2022). Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis.
D Di Stasio,D Lauritano,A Romano,C Salerno,G Minervini,G Minervini,E Gentile,R Serpico,A Lucchese (2015). In Vivo Characterization of Oral Pemphigus Vulgaris by Optical Coherence Tomography.
Leila Kheirandish-Gozal,Rakesh Bhattacharjee,Hari Bandla,David Gozal (2014). Antiinflammatory Therapy Outcomes for Mild OSA in Children.
Daniela Di Venere,Alessandra Laforgia,Daniela Azzollini,Giuseppe Barile,Andrea De Giacomo,Alessio Inchingolo,Biagio Rapone,Saverio Capodiferro,Rada Kazakova,Massimo Corsalini (2022). Calcification of the Atlanto-Occipital Ligament (Ponticulus Posticus) in Orthodontic Patients: A Retrospective Study.
A Inchingolo,I Ferrara,F Viapiano,A Netti,M Campanelli,S Buongiorno,G Latini,V Carpentiere,A Ciocia,S Ceci (2022). Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report.
L Kheirandish-Gozal,H Bandla,D Gozal (2016). Montelukast for Children with Obstructive Sleep Apnea: Results of a DoubleBlind, Randomized, Placebo-Controlled Trial.
Giovanni Coloccia,Alessio Inchingolo,Angelo Inchingolo,Giuseppina Malcangi,Valentina Montenegro,Assunta Patano,Grazia Marinelli,Claudia Laudadio,Luisa Limongelli,Daniela Di Venere,Denisa Hazballa,Maria D’oria,Ioana Bordea,Edit Xhajanka,Antonio Scarano,Felice Lorusso,Alessandra Laforgia,Francesco Inchingolo,Gianna Dipalma (2021). Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature.
S Adina,G Dipalma,I Bordea,O Lucaciu,C Feurdean,A Inchingolo,R Septimiu,G Malcangi,S Cantore,D Martin (2020). Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects.
A Ballini,S Cantore,C Altini,G Dipalma,C Ferrari,A Niccoli Asabella,G Rubini,F Inchingolo (2018). 99mTc-Diphosphonates Bone Scintigraphy for Vitality Evaluation in Cleft Palate.
Francesco Inchingolo,Marco Tatullo,Massimo Marrelli,Alessio Inchingolo,Roberto Corelli,Angelo Inchingolo,Paolo Flace,Raffaele Cagiano,Gianna Dipalma,Fabio Abenavoli (2014). Semi-open rhinoplasty: a new Maxillofacial technique.
Bita Kiaee,Ludovica Nucci,Farzin Sarkarat,Ahmad Talaeipour,Sara Eslami,Faezeh Amiri,Abdolreza Jamilian (2021). Three-dimensional assessment of airway volumes in patients with unilateral cleft lip and palate.
M Michalsky,K Reichard,T Inge,J Pratt,C Lenders (2012). American Society for Metabolic and Bariatric Surgery ASMBS Pediatric Committee Best Practice Guidelines.
N Fagundes,G Minervini,B Furio Alonso,L Nucci,V Grassia,F Apuzzo,A Puigdollers,L Perillo,C Flores-Mir (2023). Patient-reported outcomes while managing obstructive sleep apnea with oral appliances: A scoping review.
Antonino Lo Giudice,Vincenzo Quinzi,Vincenzo Ronsivalle,Marco Farronato,Carmelo Nicotra,Francesco Indelicato,Gaetano Isola (2020). Evaluation of Imaging Software Accuracy for 3-Dimensional Analysis of the Mandibular Condyle. A Comparative Study Using a Surface-to-Surface Matching Technique.
V Daniele,L Macera,G Taglieri,A Di Giambattista,G Spagnoli,A Massaria,M Messori,E Quagliarini,G Chiappini,V Campanella (2020). Thermoplastic Disks Used for Commercial Orthodontic Aligners: Complete Physicochemical and Mechanical Characterization.
S Mummolo,A Nota,F Albani,E Marchetti,R Gatto,G Marzo,V Quinzi,S Tecco (2020). Salivary Levels of Streptococcus Mutans and Lactobacilli and Other Salivary Indices in Patients Wearing Clear Aligners versus Fixed Orthodontic Appliances: An Observational Study.
S Saccomanno,V Quinzi,S Sarhan,D Laganà,G Marzo (2020). Perspectives of Tele-Orthodontics in the COVID-19 Emergency and as a Future Tool in Daily Practice.
G Minervini,R Franco,M Marrapodi,L Fiorillo,G Cervino,M Cicciù (2023). The Association between Parent Education Level, Oral Health, and Oral-Related Sleep Disturbance. An Observational Crosssectional Study.
Antonino Lo Giudice,Vincenzo Quinzi,Vincenzo Ronsivalle,Stefano Martina,Orazio Bennici,Gaetano Isola (2020). Description of a Digital Work-Flow for CBCT-Guided Construction of Micro-Implant Supported Maxillary Skeletal Expander.
M Rosa,V Quinzi,G Marzo (2019). Paediatric Orthodontics Part 1: Anterior Open Bite in the Mixed Dentition.
Enrico Marchetti,Simona Tecco,Eleonora Caterini,Fabio Casalena,Vincenzo Quinzi,Antonella Mattei,Giuseppe Marzo (2017). Alcohol-free essential oils containing mouthrinse efficacy on three-day supragingival plaque regrowth: a randomized crossover clinical trial.
Sawako Kawakami,Makoto Shiota,Kazuhiro Kon,Masahiro Shimogishi,Hajime Iijima,Shohei Kasugai (2021). Autologous micrografts from the palatal mucosa for bone regeneration in calvarial defects in rats: a radiological and histological analysis.
A Inchingolo,G Malcangi,A Inchingolo,F Piras,V Settanni,G Garofoli,G Palmieri,S Ceci,A Patano,N De Leonardis (2022). Benefits and Implications of Resveratrol Supplementation on Microbiota Modulations: A Systematic Review of the Literature.
G Malcangi,A Inchingolo,A Patano,G Coloccia,S Ceci,M Garibaldi,A Inchingolo,F Piras,F Cardarelli,V Settanni (2022). Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment-A Case Report.
Akshayraj Langaliya,Mohammad Alam,Usha Hegde,Mangesh Panakaje,Gabriele Cervino,Giuseppe Minervini (2023). Occurrence of Temporomandibular Disorders among patients undergoing treatment for Obstructive Sleep Apnoea Syndrome (OSAS) using Mandibular Advancement Device (MAD): A Systematic Review conducted according to <scp>PRISMA</scp> guidelines and the Cochrane handbook for systematic reviews of interventions.
G Minervini,L Nucci,A Lanza,F Femiano,M Contaldo,V Grassia (2020). Review for "Step‐back anterior repositioning splint retraction for temporomandibular joint disc displacement with reduction in adult patients".
E Marchetti,F Casalena,A Capestro,S Tecco,A Mattei,G Marzo (2017). Efficacy of two mouthwashes on 3‐day supragingival plaque regrowth: a randomized crossover clinical trial.
V Quinzi,G Panetta,P Filippi,F Rizzo,L Mancini,S Mummolo (2020). Autotransplatation of Immature Third Molars as Substitutes for Congenitally Missing Second Premolars: An Alternative Solution in a Young Patient with Oligodontia.
Maria Dinoi,Enrico Marchetti,Umberto Garagiola,Silvia Caruso,Stefano Mummolo,Giuseppe Marzo (2016). Orthodontic treatment of an unerupted mandibular canine tooth in a patient with mixed dentition: a case report.
S Mummolo,A Nota,E Marchetti,G Padricelli,G Marzo (2016). The 3D Tele Motion Tracking for the Orthodontic Facial Analysis.
Vincenzo Quinzi,Sabina Saccomanno,Rebecca Manenti,Silvia Giancaspro,Licia Coceani Paskay,Giuseppe Marzo (2020). Efficacy of Rapid Maxillary Expansion with or without Previous Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Syndrome Based on Polysomnographic Data: A Systematic Review and Meta-Analysis.
M Pasini,M Giuca,S Ligori,S Mummolo,F Fiasca,G Marzo,V Quinzi (2020). Association between Anatomical Variations and Maxillary Canine Impaction: A Retrospective Study in Orthodontics.
Sara Caruso,Emanuela Lisciotto,Silvia Caruso,Alessandra Marino,Fabiana Fiasca,Marco Buttarazzi,David Sarzi Amadè,Melania Evangelisti,Antonella Mattei,Roberto Gatto (2023). Effects of Rapid Maxillary Expander and Delaire Mask Treatment on Airway Sagittal Dimensions in Pediatric Patients Affected by Class III Malocclusion and Obstructive Sleep Apnea Syndrome.
A Yoon,M Abdelwahab,R Bockow,A Vakili,K Lovell,I Chang,R Ganguly,S Liu,-C Kushida,C Hong,C (2022). Impact of Rapid Palatal Expansion on the Size of Adenoids and Tonsils in Children.
Paola Pirelli,Maurizio Saponara,Christian Guilleminault (2015). Rapid maxillary expansion (RME) for pediatric obstructive sleep apnea: a 12-year follow-up.
M Villa,A Rizzoli,J Rabasco,O Vitelli,N Pietropaoli,M Cecili,A Marino,C Malagola (2015). Rapid Maxillary Expansion Outcomes in Treatment of Obstructive Sleep Apnea in Children.
Paola Pirelli,Ezio Fanucci,Aldo Giancotti,Michele Di Girolamo,Christian Guilleminault (2019). Skeletal changes after rapid maxillary expansion in children with obstructive sleep apnea evaluated by low-dose multi-slice computed tomography.
P Pirelli,V Fiaschetti,E Fanucci,A Giancotti,' Condo,R Saccomanno,S Mampieri,G (2021). Cone Beam CT Evaluation of Skeletal and Nasomaxillary Complex Volume Changes after Rapid Maxillary Expansion in OSA Children.
J Kim,K Hwang,S Kim,S Liu,S Kim (2022). Correlation between Craniofacial Changes and Respiratory Improvement after Nasomaxillary Skeletal Expansion in Pediatric Obstructive Sleep Apnea Patients.
L.-C Chuang,Y.-J Hwang,Y.-C Lian,M Hervy-Auboiron,P Pirelli,Y.-S Huang,C Guilleminault (2019). Changes in Craniofacial and Airway Morphology as Well as Quality of Life after Passive Myofunctional Therapy in Children with Obstructive Sleep Apnea: A Comparative Cohort Study.
Swapnil Ghodke,Ashok Utreja,Satinder Singh,Ashok Jena (2014). Effects of twin-block appliance on the anatomy of pharyngeal airway passage (PAP) in class II malocclusion subjects.
P Keerthana,G Negi,P Chitra (2022). Airway Changes in Patients with Sleep Apnea Using AdvanSync2 Class II Correctors-A Case Series.
A Machado-Junior,L.-G Signorelli,E Zancanella,A.-N Crespo (2016). Randomized controlled study of a mandibular advancement appliance for the treatment of obstructive sleep apnea in children: A pilot study.
Cynthia Medina,Hiroshi Ueda,Koji Iwai,Ryo Kunimatsu,Kotaro Tanimoto (2022). Changes in airway patency and sleep-breathing in healthy skeletal Class II children undergoing functional Activator therapy.
Chen Zhang,Hong He,Peter Ngan (2013). Effects of twin block appliance on obstructive sleep apnea in children: a preliminary study.
Tingting Zhao,Peter Ngan,Fang Hua,Jie Zheng,Shunquan Zhou,Man Zhang,Hui Xiong,Hong He (2018). Impact of pediatric obstructive sleep apnea on the development of Class II hyperdivergent patients receiving orthodontic treatment:.
M Zreaqat,R Hassan,A Samsudin,S Alforaidi (2023). Effects of Twin-Block Appliance on Upper Airway Parameters in OSA Children with Class II Malocclusion and Mandibular Retrognathia: A CBCT Study.
Hui Chen,Alan Lowe (2013). Updates in oral appliance therapy for snoring and obstructive sleep apnea.
Fabrizia D’apuzzo,Ludovica Nucci,Ines Delfino,Marianna Portaccio,Giuseppe Minervini,Gaetano Isola,Ismene Serino,Carlo Camerlingo,Maria Lepore (2021). Application of Vibrational Spectroscopies in the Qualitative Analysis of Gingival Crevicular Fluid and Periodontal Ligament during Orthodontic Tooth Movement.
Giuseppe Minervini,Rocco Franco,Maria Marrapodi,Luca Fiorillo,Gabriele Cervino,Marco Cicciù (2023). Prevalence of temporomandibular disorders in children and adolescents evaluated with Diagnostic Criteria for Temporomandibular Disorders: A systematic review with meta‐analysis.
Giuseppe Minervini,Rocco Franco,Maria Marrapodi,Salvatore Crimi,Almir Badnjević,Gabriele Cervino,Alberto Bianchi,Marco Cicciù (2023). Correlation between Temporomandibular Disorders (TMD) and Posture Evaluated trough the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD): A Systematic Review with Meta-Analysis.
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.




































































