Assessment of Levels of Immunization and Factors Associated with the Non-completion Routine Immunization within (9-12 Months) Attending Primary Healthcare Centres in Ibadan North and South East, Nigeria
Immunization is designed to prevent transmittable diseases and it is an integral public medical intervention and an economical method to decline mortality and morbidity associated with transmittable diseases. This work attempts to determine the vaccine coverage and factors related to the non-completion routine immunization within babies (9-12 months) attending Primary Healthcare Centre (PHC) in Ibadan North and South East Local Government Areas, Oyo State.
Basiru $\alpha$, T. A., Ogunwale $\sigma$, T. O., Oluwalana $\rho$, A. I., Oladele, D. O., Oyetola $\yen$, S. O., Ibrahim $\S$, D. O., Oladimeji $\chi$, J. F., Abbah $\nu$, S. C., Ekanade $\theta$, C. T. & Balogun $\zeta$, F. A.
## I. INTRODUCTION
Immunization denotes building up people's immune response against an agent. Immunization is a more accessible means to get immune to a particular disease, and it is less hazardous (Fiore et al., 2019). Vaccines are necessary for both infants and of ages because they defend against the several diseases. Aside from defending infants against life-limiting illnesses, immunization as well assists in building body's defences of infants (Fiore et al., 2019). The prescription of a vaccine to help the immune response build defense against diseases is termed vaccination. Vaccines comprise a microbe or virus in a destroyed or weakened condition, or proteins or toxins from the living organism.
Immunization of children against six preventable diseases (diphtheria, pertussis, tuberculosis, polio, tetanus, and measles) is essential to decline childhood morbidity and fatality. Immunization continues to be one of the most cost-efficient and integral public healthcare interventions to reduce child morbidity and mortality. Globally, childhood vaccination is projected to prevent from 2 to 3 million mortalities yearly (Meleko et al., 2017). Using immunizations, a few infectious diseases have been eliminated in most regions of the Earth planet. One instance of such is smallpox and poliomyelitis. Polio is still common in a few nations of the earth and a few people might still be at menace of contacting it, particularly those who have never received the vaccine, people who didn't obtain all doses of the vaccine, and those that journey to regions of the earth in which polio is still rampant. Immunization is a proven device efficient to prevent and eliminate transmittable diseases. The WHO conducted an immunization crusade between 1967 and 1977 and it led to the eradication of smallpox.
At the beginning of programme, smallpox still threatened $60\%$ of the earth's population. Likewise, the destruction of poliomyelitis is presently possible. Since the inauguration via WHO and its partners of the Global Polio Eradication Initiative in 1988, infection has dropped by $99\%$, and nearly five million individuals eluded paralysis. It was predicted that from year 2000 to 2008, measles mortalities worldwide fallen by above $78\%$, in regions of the earth established a goal to eradicate prevalence of polio disease. Neonatal and maternal tetanus have been eliminated from 20 of the 58 heavy-risk nations (Masresha et al., 2018).
In man's history, the development and broad dissemination of childhood vaccines have been one of the ultimate successes of public health. Initiatives like Expanded Programme on Immunization (EPI) through WHO promoted coordinated, nation-level development in routine vaccination (e.g., tetanus, diphtheria, pertussis, polio, measles, and BCG), and laid the roots for attempts to bring in fresh vaccines and further increase coverage over the future decade. The EPI continues to be devoted to its aim of global access to all crucial vaccines (Masresha et al., 2018).
Empirical reviews have indicated that the mortality of children takes place more often in the growing countries. Essentially, children residing in African nations die yearly as a result of avoidable transmittable diseases. Similarly, Epidemiological accounts in African zones indicate 'nine million mortalities of children globally due to vaccine-avoidable diseases (Masresha et al., 2018), and a greater percentage which is 4.4 million happened in sub-Saharan Africa'. This is considerably attributed to weak immunization coverage and health problems in sub-Saharan Africa. Furthermore, in many areas of Africa, immunization facilities have not been ideal, especially for routine immunization which is known as the critical factor for below vaccination of children (Hill et al., 2021).
In 2017, around $20\%$ of babies in the globe with incomplete DPT immunization lived in Nigeria (Obanewa et al., 2020), and three million out of the projected 8.9 million children in the WHO African Zone who were not vaccinated against measles in 2015 are residing in Nigeria (Obanewa et al., 2020). Therefore, Nigeria represents nearly $40\%$ of the 28279 measles cases stated in the WHO African Zone in 2016 (Masresha et al., 2017). Nigeria has a yearly population growth rate of $2.83\%$ which makes Nigeria the most thickly populated nation in Africa and is the second most significant factor contributory to below-five fatality universally (Masresha et al., 2018). There are marked differences across geopolitical regions with vaccination coverage and completion, which vary from around $50\%$ in the South-South and South-West to 27, 14, and $10\%$ in the North-East, North-Central, and North-West Nigeria, respectively (Masresha et al., 2017).
All states in Nigeria fall under the global goal of $80\%$ coverage for three doses of pentavalent immunization. Performance level of immunization is poorest in North West or North East areas where all the states falls under $50\%$ pentavalent coverage. Children residing in the rural areas are half as possibly to be immunized than those in built-up areas and children of younger and less educated caretakers are at most threat (Hill et al., 2021).
Immunization is a vital vision of the PHC system in Nigeria. One of the significant aspects emphasized by the worldwide community is accomplishing global health coverage, and PHC is a needed foundation for these endeavors. Vaccination is an integral part of international health coverage, which is fundamental to PHC. Nevertheless, a few factors like medical distrust, sociopolitical factors, unfriendly behaviours of medical personnel, poor medical systems, clashes between programmes, and supplementary immunization activities are contributing factors that hinder sufficient immunization coverage in PHCs (Masresha et al., 2017; Hill et al., 2021).
An investigation on rural-urban disparities in demographic factors and related immunization status among children of 12-59 months in a south-western region of Nigeria indicates that immunization coverage was relatively high but yet substandard in the southwestern part of Nigeria (Ijarotimi et al., 2018). Maternal factors were observed to control immunization status. Other factors in line with the research are location and paternal factors, which are highly related to immunization coverage in the south-western zone of Nigeria. Also, in Oyo State, a survey on unacceptable rates of immunization coverage in governmental recognized factors related to the accomplishment of a total child vaccination schedule in Ido LGAs and Ibadan North East (LGAs) of Oyo State, Nigeria (Fatiregun et al., 2013). The investigation revealed that the status of complete immunization coverage was unacceptable in nearly all the clinic wards (Fatiregun et al., 2013).
Immunization is vital in the prevention of infectious and poor immunization is ascribed to some diseases in little one; hence, it is crucial to evaluate factors that result in non-completion routine immunization in little one. Depending on this proposition, the purpose of this study was to investigate the level of vaccination and factors accountable for non-completion routine immunization within (9-12 months) attending PHCs in Ibadan North and South East LGAs, Oyo State, Nigeria and offer lasting solution recommendations to the challenge of incomplete immunization status.
## II. MATERIALS AND METHODS
Descriptive cross-sectional analysis was carried out on mothers/caregivers who attended immunization programs in Ibadan North and South East Local Government, Oyo State, Nigeria during November 2019-April 2020. Depending on geographical areas, the study site was separated into two zones: Ibadan North and Ibadan South East. Then the three PHCs each from both Ibadan North and South East LGAs were randomly chosen from this zones and sampling was conducted utilizing multistage sampling technique. The work was approved by the Research Ethics Review Committee of Department of Planning, Research, and Statistics Division, Ministry of Health, Oyo State, Nigeria (codenumber: AD 13/479/4307A) and written informed consent was obtained from all the participants. After explaining the objectives of the research, the questionnaires were completed by the subjects or researcher in case of illiteracy of the participants. Inclusion criteria were being an all mother/caregiver with children between 9 and 12 months attending immunization clinic at the chosen PHCs in Ibadan North and South East LGA, and those that tend to participate in the investigation. Exclusion criteria were mother/caregiver with children having health problems resulting in hospitalization. The sample size of the survey was estimated as 422 utilizing the Cochran formula the unidentified population, with a standard deviation of the score being 10 $(\sigma = 10)$, the error value of 1 $(d = 1)$, type I error $(\alpha =.05$, $z = 1.96)$ taking into consideration a $10\%$ attrition.
### a) Data Collection
Four questionnaires were employed for data gathering as follows: (i) socio-demographic factors of participants; (ii) child immunization coverage; (iii) knowledge, perceptions, and attitude towards child vaccination; and (iv) associated factors with child vaccination coverage in PHCs'.
### b) Demographic Questionnaire
The demographic factors form comprised nine items regarding age, marital status, education qualification, number of children, occupation, monthly earnings, religion, ethnicity, and baby's age.
### c) Child Immunization Coverage Questionnaire
The child immunization coverage questionnaire was a researcher-made tool comprising thirteen items. The items covered the areas of vaccinating the child after birth is a piece of common knowledge among mothers in our local government area; we, don't think there is adequate immunization coverage in health clinics within my community; all, statutory child vaccines are readily available in health clinics within my community, has your child ever received polio, measles, pneumococcal (PMV) vaccine, yellow fever, and pentavalent immunizations? Has your child ever received any vaccinations, drops, or injections in the past?, Has your child ever received an injection in the right upper arm or shoulder that usually results in a scar? The vaccine is not available in many clinics in my community, where does your child usually receive vaccinations? Where did your child receive their most recent vaccination?
The validity of the questionnaire was confirmed by an authorized letter of introduction from the Department of Public Health, Faculty of Basic and Medical Science, Lead City University, Ibadan, by interviewing technique employing KoBo collect androids application in each LGA by the researcher with the assistance of trained research assistants who were students from colleges of Health Technology with the support of health officers working in the chosen centers picked for the investigation. Also, the test-retest reliability was determined by giving the questionnaire to 10 eligible people in two rounds with a14-day duration. The Chi-square was calculated as 23.544 and 27.528, which were significantly different at the $p < 0.001$.
### d) The Measure of Parental/Caregivers' Knowledge and Misperceptions of Routine Immunization Questionnaire
The questionnaire comprises ten questions, and the questions dealt with the areas of childhood vaccines are vital for my child's health, getting vaccines is a good way to protect our child/children from diseases, measles vaccine needs to be obtained at nine months, vaccination schedule needs to be completed before twelve months?, oral polio ought to be received three times?, several communities and caregivers reject RI because of rumors, false information, and fear, lack of confidence and trust in RI as effective health interventions seem to be pretty common in all regions of Nigeria; RI, is to depopulate the society; RI will make their children infertile when they grow up, and we are afraid that our child/children will be affected with virus.
### e) Associated Factors with Child Immunization Coverage in Primary Healthcare Centers Questionnaire
The questionnaire involved fourteen questions and contained three sublevels comprising why the child was not vaccinated, why the child hasn't had all recommended vaccines, and health officers' attitudes. This questionnaire measured the associated factors with child immunization coverage and determine of medical worker attitude. The overall knowledge level for child vaccination was estimated as the composite of five knowledge questions, which comprised whether the participants knew the significance of vaccine to health, whether the vaccine is a suitable means to defend the child from disease, knowledge of the age measles vaccine needs to be given, awareness on whether vaccination has to be completed before 12 months, and the number of times polio vaccines needs to be given.
Those who had the correct answer to each knowledge questions were graded 1 point and those who didn't know were graded 0 point. The knowledge mark was estimated as the sum of all knowledge questions with a lowest mark of 0 and highest mark of 5. The knowledge status of participants was classified as good knowledge when participants grade was more significant than the average mark (which was 2), and poor knowledge when grade was below the average mark. Depending on the total mark in this questionnaire, the samples were categorized as negative perception concerning RI (1 mark) and positive perception regarding RI (0 mark) groups. The validity and reliability of this instrument were approved in research conducted by the WHO
Vaccination Coverage Survey published in 2018 and reviewed in 2019 (NDHS, 2019). Furthermore, the authors evaluated the reliability and validity of this instrument in Nigeria by interviewing procedure utilizing the KoBo collect androids application (Hill et al., 2021). In this work, the validity of this questionnaire was estimated using the informed content validity. For this the questionnaire was submitted to 10 experts, the confirmation of whom was indicative of approved informed content validity. More so, intending to measure the reliability of the questionnaire, ten eligible people completed the questionnaire in two rounds with 14 days. By the way, the Chi-square between the questionnaire marks was found to be 23.544 and 27.528.
 Fig. 1: Field Sampling from the Researcher from One of the PHCs in Ibadan
### f) Data Analysis
Statistical analysis was conducted utilizing SPSS software (Statistical Package for the Social Sciences, version 21.0, SPSS Inc., Chicago, Illinois, USA). We used descriptive (e.g., frequency, mean, standard deviation, percentage, bar, and pie charts) and inferential (e.g., regression analysis) statistics. Lastly, $p < 0.05$ was regarded as significantly different.
## III. RESULTS
### a) Search Results and Survey Characteristics
Socio-demographic characteristics of the study participants: 422 mothers/caregivers of children aged 9 to 12 months were involved in this work. The age of the respondents varied between 14 and 34 years, with an average of $29 \pm 6.17$ years. The most represented age class was 24 to 28 (37.9%). The proportion of the study population following the study geographical distribution was $54\%$ for Ibadan South East while $46\%$ for Ibadan North LGA. Among the PHCs, 115 (27.3%) were Boluwaji PHC. Four hundred and seven (97.4%) mothers/caregivers were married, 6 (1.4%) were single, and 4 (1.0%) were widowed/separated/cohabiting. One hundred and twenty-two $(28.9\%)$ mothers/caregivers' had a level of education at least equivalent to a secondary school certificate, while 93 $(22\%)$, 87 $(20.6\%)$, 42 $(10\%)$, 49 $(11.6\%)$, and 2 $(0.5\%)$ stated possessing a primary school certificate, OND, HND, BSc, and Postgraduate certificates, and 27 $(6.4\%)$ had no formal education. Of the 422 participants involved in this assessment, 146 $(34.6\%)$, 242 $(57.3\%)$, and 34 $(8.1\%)$ had 1 to 2 children, 3-4 children, and five and more children, respectively. Concerning occupation, 203 $(48.6\%)$ study participants were traders. About religion, 174 $(41.2\%)$ were Christian, 241 $(57.1\%)$ were Islam, while 7 $(1.7\%)$ were other religions; 41.3% of the study population had a mean monthly income of between 0 and 18,000 Naira; the most common ethnic group in the study population was Yoruba $(69\%)$. There was a significant relationship between age group, marital level, academic status of females, women's employment level, women's monthly income, number of children, religions, and ethnic status. Details of the sociodemographic profile of the respondents are shown in Table 1.
Table 1: Summary of Measure of Demographic Variables based on Descriptive Statistics The number of participants=422
<table><tr><td>Attributes</td><td colspan="2">Frequency (n)</td><td>Percentage (%)</td></tr><tr><td colspan="4">Mean age: 29.29 ± 6.17</td></tr><tr><td colspan="4">Age group</td></tr><tr><td>14 to 18 years</td><td>11</td><td></td><td>2.6</td></tr><tr><td>19 to 23 years</td><td>43</td><td></td><td>10.2</td></tr><tr><td>24 to 28 years</td><td>160</td><td></td><td>37.9</td></tr><tr><td>29 to 33 years</td><td>108</td><td></td><td>25.6</td></tr><tr><td>34 years and above</td><td>100</td><td></td><td>23.7</td></tr><tr><td>Total</td><td>422</td><td></td><td>100.0</td></tr><tr><td colspan="4">LGA</td></tr><tr><td>Ibadan North</td><td>194</td><td></td><td>46.0</td></tr><tr><td>Ibadan Southeast</td><td>228</td><td></td><td>54.0</td></tr><tr><td>Total</td><td>422</td><td></td><td>100.0</td></tr><tr><td colspan="4">Primary Health Centre</td></tr><tr><td>Idi Ogungun PHC</td><td>103</td><td></td><td>24.4</td></tr><tr><td>Agbowo PHC</td><td>52</td><td></td><td>12.3</td></tr><tr><td>Basorun PHC</td><td>39</td><td></td><td>9.2</td></tr><tr><td>Molete PHC</td><td>71</td><td></td><td>16.8</td></tr><tr><td>Algon Comprehensive PHC</td><td>42</td><td></td><td>10.0</td></tr><tr><td>Boluwaji PHC</td><td>115</td><td></td><td>27.3</td></tr><tr><td>Total</td><td>422</td><td></td><td>100.0</td></tr><tr><td colspan="4">Marital Level</td></tr><tr><td>Single</td><td>6</td><td></td><td>1.4</td></tr><tr><td>Married</td><td>407</td><td></td><td>97.4</td></tr><tr><td>Cohabiting</td><td>1</td><td></td><td>.2</td></tr><tr><td>Widowed/separated/cohabiting</td><td>4</td><td></td><td>1.0</td></tr><tr><td>Total</td><td>418</td><td></td><td>100.0</td></tr><tr><td colspan="4">Academic Status</td></tr><tr><td>No formal education</td><td>27</td><td></td><td>6.4</td></tr><tr><td>Primary school leaving certificate</td><td>93</td><td></td><td>22.0</td></tr><tr><td>Secondary school certificate</td><td>122</td><td></td><td>28.9</td></tr><tr><td>OND</td><td>87</td><td></td><td>20.6</td></tr><tr><td>HND</td><td>42</td><td></td><td>10.0</td></tr><tr><td>BSC</td><td>49</td><td>11.6</td></tr><tr><td>Postgraduate</td><td>2</td><td>0.5</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td>Number of Children</td><td></td><td></td></tr><tr><td>1-2 Children</td><td>146</td><td>34.6</td></tr><tr><td>3-4 Children</td><td>242</td><td>57.3</td></tr><tr><td>Five or more Children</td><td>34</td><td>8.1</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td>Occupation</td><td></td><td></td></tr><tr><td>Housewife</td><td>66</td><td>15.8</td></tr><tr><td>Trader</td><td>203</td><td>48.6</td></tr><tr><td>Artisan</td><td>35</td><td>8.4</td></tr><tr><td>Skilled worker</td><td>53</td><td>12.7</td></tr><tr><td>Civil servant</td><td>59</td><td>14.1</td></tr><tr><td>Other, identify</td><td>2</td><td>0.5</td></tr><tr><td>Total</td><td>418</td><td>100.0</td></tr><tr><td>Monthly Income (Naira)</td><td></td><td></td></tr><tr><td>0 - 18,0000</td><td>173</td><td>41.3</td></tr><tr><td>19,000-40,000</td><td>126</td><td>30.1</td></tr><tr><td>41,000-60,000</td><td>52</td><td>12.4</td></tr><tr><td>61,000-80,000</td><td>33</td><td>7.9</td></tr><tr><td>81,000 and above</td><td>35</td><td>8.4</td></tr><tr><td>Total</td><td>419</td><td>100.0</td></tr><tr><td>Religion</td><td></td><td></td></tr><tr><td>Christianity</td><td>174</td><td>41.2</td></tr><tr><td>Islam</td><td>241</td><td>57.1</td></tr><tr><td>Others</td><td>7</td><td>1.7</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td>Ethnic Status</td><td></td><td></td></tr><tr><td>Yoruba</td><td>292</td><td>69.2</td></tr><tr><td>Igbo</td><td>49</td><td>11.6</td></tr><tr><td>Hausa</td><td>77</td><td>18.2</td></tr><tr><td>Others</td><td>4</td><td>0.9</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr></table>
### b) Coverage of Childhood Immunization in the two Lgas In Ibadan Primary Healthcare Centers
Immunization coverage of children aged 9 to 12 months in the two LGA in Ibadan Primary Healthcare Centres of the 422 children aged 9 to 12 months involved in this survey, $77.7\%$ received polio immunization, $62.3\%$ obtained measles immunization, $66.8\%$ obtained pneumococcal immunization, $59.2\%$ had yellow fever vaccination, $78.2\%$ obtained pentavalent vaccination, $89.3\%$ received any vaccination drops or injections in the past. In contrast, $84.4\%$ received injection in the right upper arm (Figures 2-8).
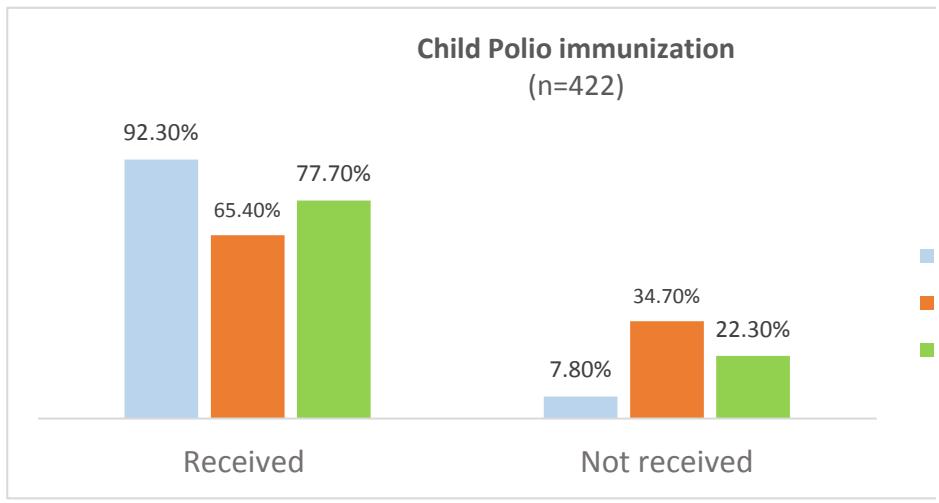
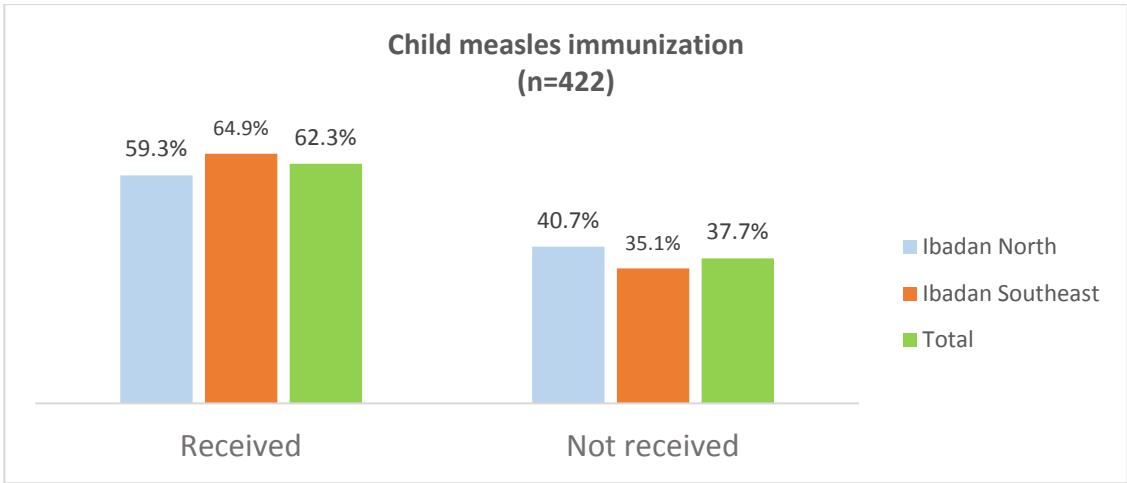
Figure 2: Percentage of Children Reported to Have Ever Received Polio Immunization by Study Geography
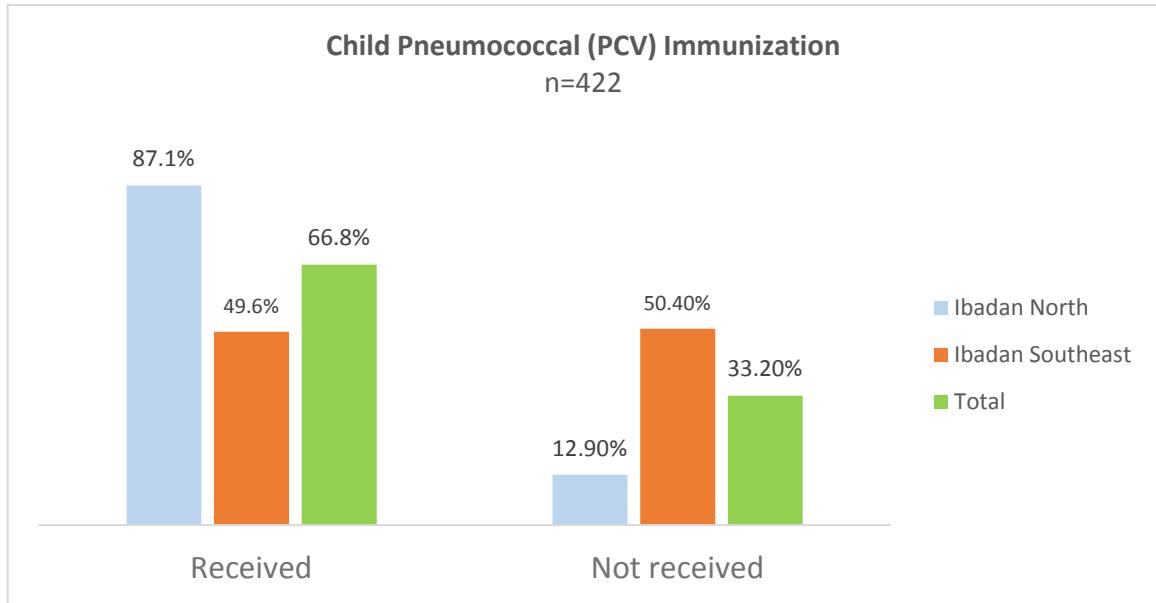
Figure 3: Percentage of Children Stated to Have Ever Received Measles Immunization by Study Geography
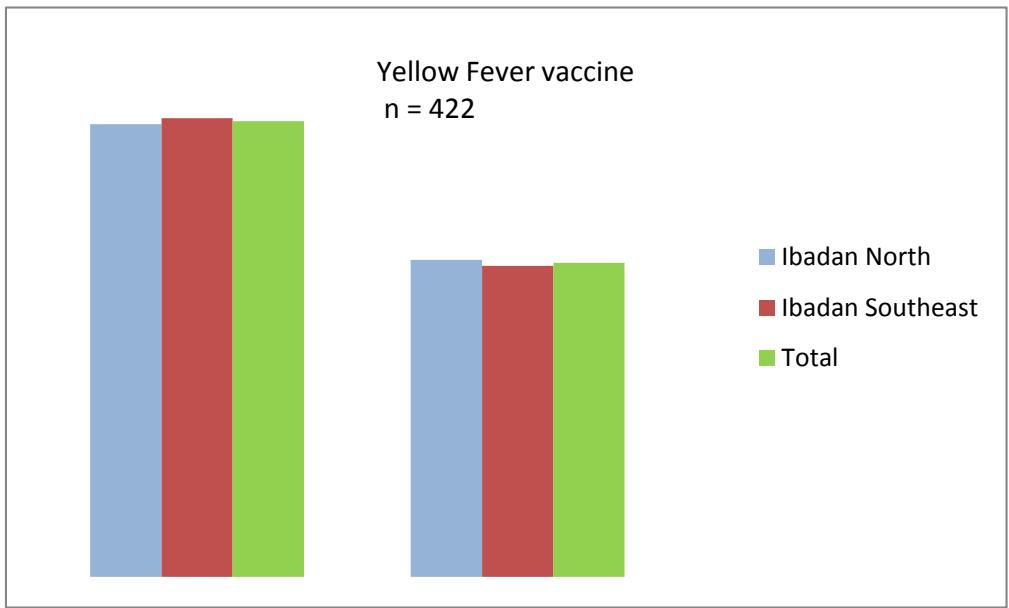
Figure 4: Percentage of Children Reported to Have Ever Received Pneumococcal (PCV) Immunization by Study Geography
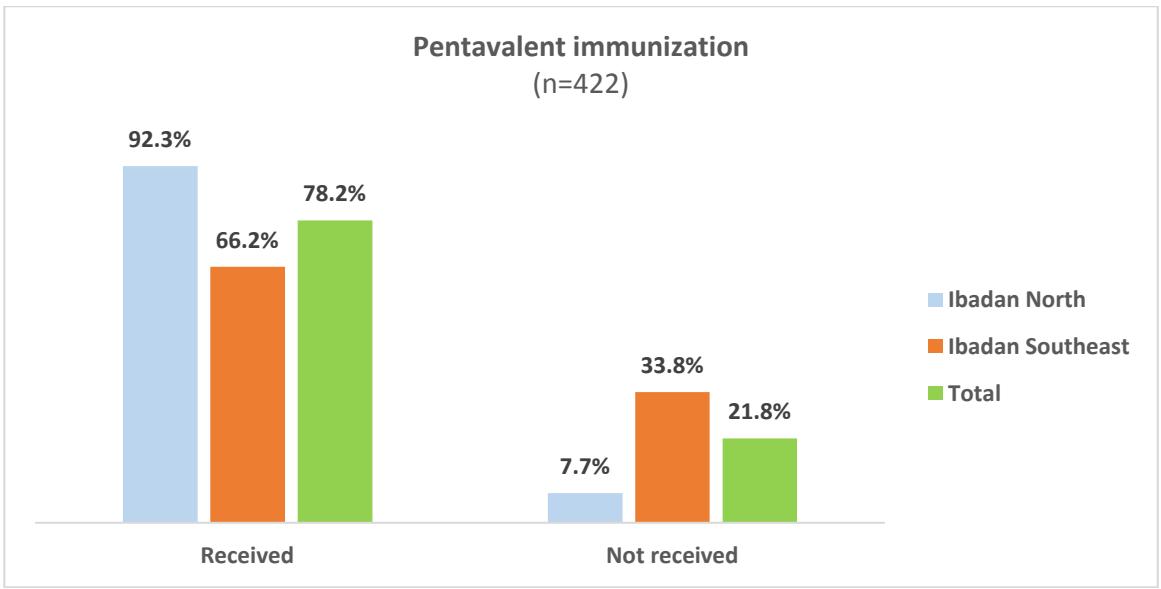
Figure 6: Percentage of Children Reported to Have Ever Received Pentavalent Immunization by Study Geography
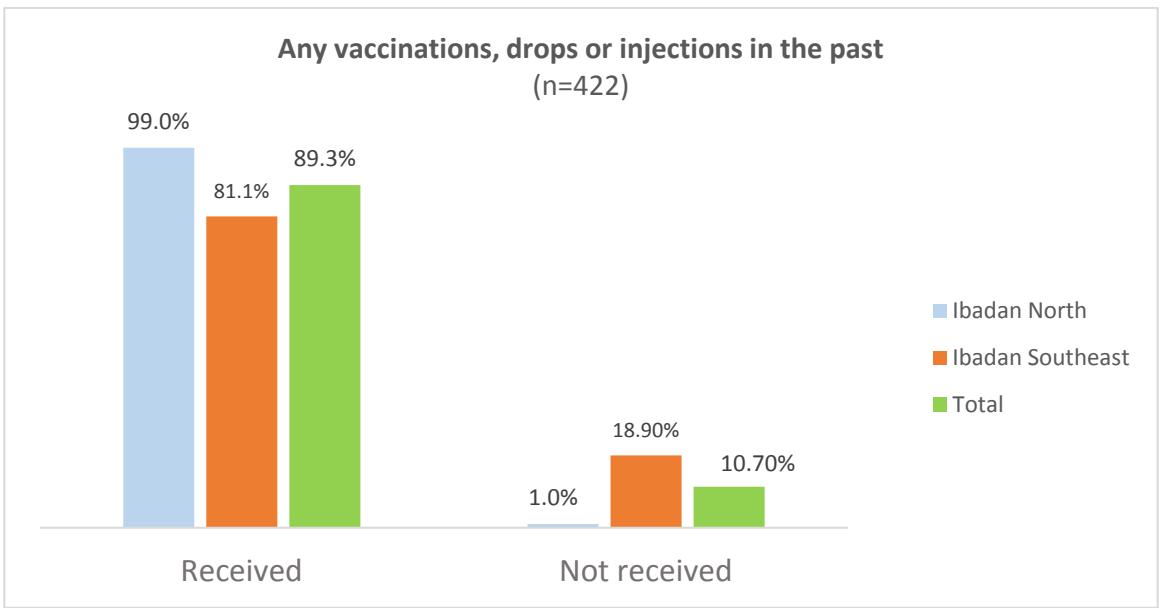
Figure 7: Percentage of Children Reported to Have Ever Received any Vaccinations, Drops, or Injections in the Past by Study Geography
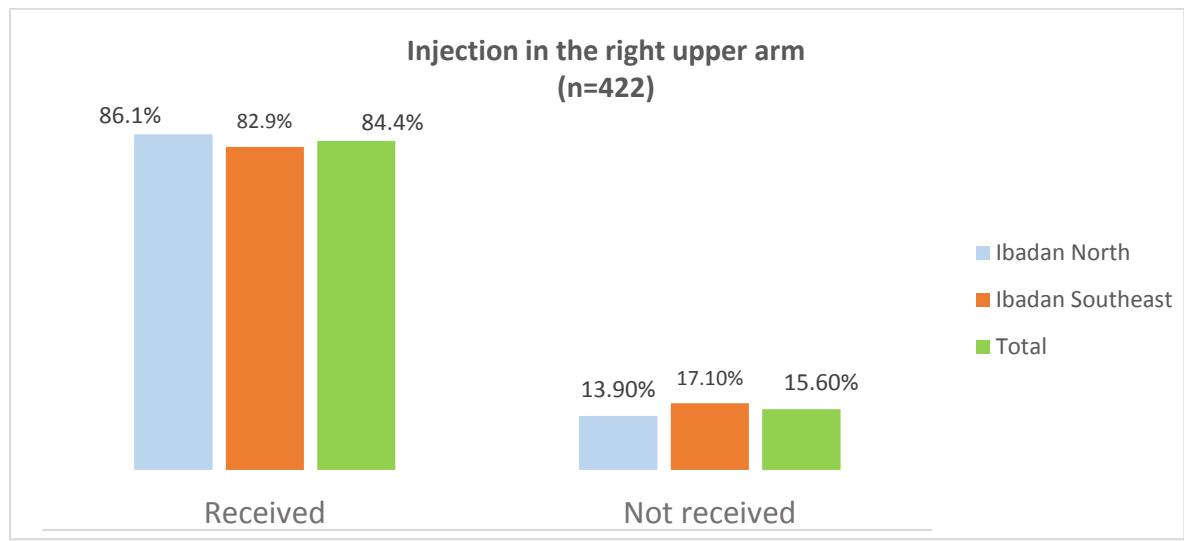 Figure 8: Percentage of Children Reported to Have Ever Received any Injection in the Right Upper Arm (Measles Vaccine) in the Past by Study Geography
Missed immunization was determined employing the five scheduled immunization. Out of 422 children within 9 - 12 months, 90 (21.3%) missed at least one of expected scheduled immunization and was high among children that are 12 months (see Table 2). Reasons for missed vaccination of mothers of children aged 9 to 12 months who were not or partially vaccinated in the Ibadan healthcare centers in 2022.
Ninety mothers/caregivers of children aged 9 to 12 months who were not or partially vaccinated gave the reasons for not vaccinating of their child. Visits to the clinic were not on the date of vaccination (32% and 51%), the child fell sick (46% and 24%), there was no vaccine (7% and 12%), and waiting was too much (4% and 7%) were the four reasons most often mentioned (Table 2).
Table 2: Summary of Missed Immunization Schedule based on Child's Age
<table><tr><td>Sn</td><td>Child's Age</td><td>Nos of Child</td><td>Nos. of Missed</td><td>% missed</td><td>Nos. vaccinated</td><td>% vaccinated</td></tr><tr><td>1</td><td>Nine months</td><td>94</td><td>2</td><td>2.1</td><td>92</td><td>97.9</td></tr><tr><td>2</td><td>Ten months</td><td>72</td><td>7</td><td>9.7</td><td>65</td><td>90.3</td></tr><tr><td>3</td><td>Eleven months</td><td>154</td><td>47</td><td>30.5</td><td>107</td><td>69.5</td></tr><tr><td>4</td><td>Twelve months</td><td>102</td><td>34</td><td>33.3</td><td>68</td><td>66.7</td></tr><tr><td></td><td>Total</td><td>422</td><td>90</td><td></td><td>332</td><td></td></tr></table>
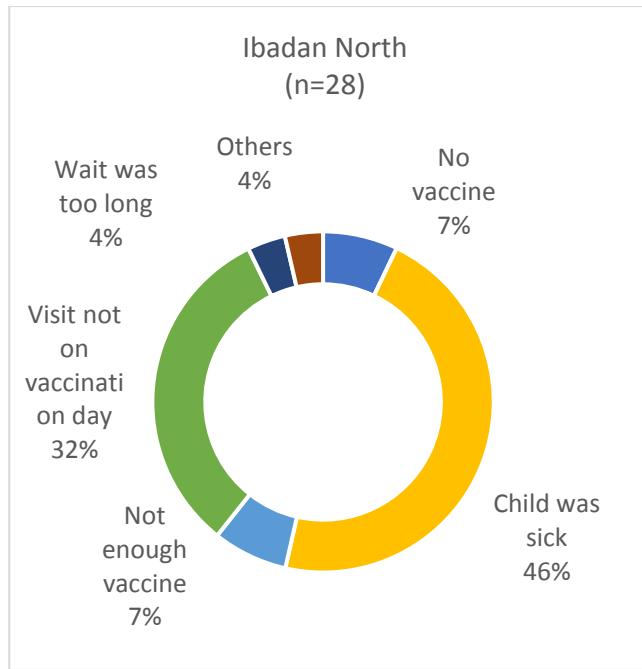
Figure 5: Percentage of Children Reported to Have Ever Received Child Yellow Fever Vaccine by Study Geography
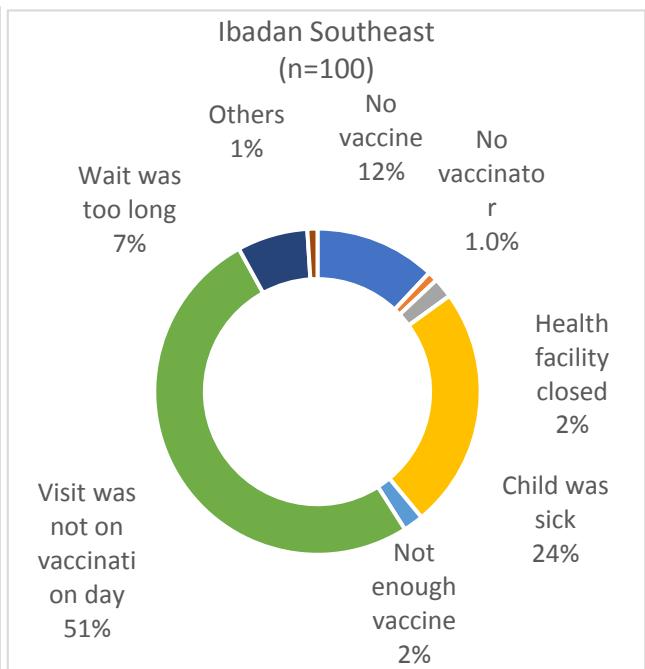 Figure 9: Reasons for Missing Vaccination of Children in both Study Locations
### c) Summary of Caregiver and Child Immunization Characteristics
Caregiver and child immunization characteristics are classified into five subtitles: (i) vaccinating the child after birth is a piece of common knowledge among mothers; (ii) no adequate immunization coverage in health clinics within the community; (iii) all statutory child vaccines are readily available in health clinics within the community; (iv) place of usual child vaccinations; and (v) place of most recent child vaccination (see Table 3). They are classified by frequency of inclusion in the assessments examined, denoted 'n'. In precis, the most often recognized factors for evaluating caregiver and child munization characteristics were: vaccinating the child after birth agree (n = 187, 44.3%); no adequate immunization coverage in health clinics agree (n = 209, 49.5%); all statutory child vaccines are readily available in health clinics agree (n = 158, 37.4%); place of usual child vaccinations (n = 407, 96.4%); and place of most recent child vaccination (n = 401, 95%).
Table 3: Summary of Caregiver and Child Immunization Characteristics
<table><tr><td>Variables</td><td>Frequency (n)</td><td>Percentage (%)</td></tr><tr><td colspan="3">Vaccinating the child after birth is a piece of common knowledge among mothers.</td></tr><tr><td>Strongly agree</td><td>96</td><td>22.7</td></tr><tr><td>Agree</td><td>187</td><td>44.3</td></tr><tr><td>Neither agree nor disagree</td><td>5</td><td>1.2</td></tr><tr><td>Disagree</td><td>132</td><td>31.3</td></tr><tr><td>Strongly disagree</td><td>2</td><td>0.5</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">There is no adequate immunization coverage in health clinics within the community</td></tr><tr><td>Strongly agree</td><td>48</td><td>11.4</td></tr><tr><td>Agree</td><td>209</td><td>49.5</td></tr><tr><td>Neither agree nor disagree</td><td>13</td><td>3.1</td></tr><tr><td>Disagree</td><td>151</td><td>35.8</td></tr><tr><td>Strongly disagree</td><td>1</td><td>0.2</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">All statutory child vaccines are readily available in health clinics within the community</td></tr><tr><td>Strongly agree</td><td>67</td><td>15.9</td></tr><tr><td>Agree</td><td>158</td><td>37.4</td></tr><tr><td>Neither agree nor disagree</td><td>10</td><td>2.4</td></tr><tr><td>Disagree</td><td>185</td><td>43.8</td></tr><tr><td>Strongly disagree</td><td>2</td><td>0.5</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">Place of usual child vaccinations</td></tr><tr><td>Local government health clinic</td><td>407</td><td>96.4</td></tr><tr><td>Local private doctor's office</td><td>4</td><td>0.9</td></tr><tr><td>Secondary healthcare facility</td><td>2</td><td>0.5</td></tr><tr><td>In a private healthcare facility</td><td>9</td><td>2.1</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">Place of most recent child vaccination</td></tr><tr><td>Local government health clinic</td><td>401</td><td>95</td></tr><tr><td>Local private doctor's office</td><td>8</td><td>1.9</td></tr><tr><td>Secondary healthcare facility</td><td>2</td><td>0.5</td></tr><tr><td>In a private healthcare facility</td><td>11</td><td>2.6</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr></table>
d) Summary of Parental/Caregivers Knowledge, Perceptions, and Attitude towards Child Vaccination
## i. Summary of Participant's Knowledge of Child Vaccination
Most knowledge and misperceptions were assessed as part of a multi-factorial approach to increase childhood vaccination coverage and were identified as adequate by the respective study authors. Specific expertise and misperceptions are classified into six subheadings: (i) childhood vaccines are essential for a child's health; (ii) getting vaccines is a good way to protect children from diseases; (iii) measles vaccine is received at nine months; (iv) vaccination schedule should be completed by twelve months; and (v) oral polio should be received three times (see Table 4). They are computed by frequency in the incorporated works, termed below as 'n'. In a nutshell, the most generally mentioned knowledge comprised childhood vaccines are essential for child's health (n = 297, 70.4%); getting vaccines is a good way to protect children from diseases (n = 329, 77.9%); measles vaccine is received at nine months (n = 244, 57.9%); vaccination schedule needs to be completed by twelve months (n = 161, 38.2); and oral polio must be received three times (n = 224, 53.1%). In general, expertise was estimated with the composite immunization knowledge score of participants, which indicated 41% for high knowledge and 59% for low knowledge regarding immunization. Higher knowledge was found among participants in Ibadan North (52.6%) than in Ibadan South East (31.1%).
Table 4: Summary of Participant's Knowledge Profile on Child Vaccination
<table><tr><td>Variables</td><td>Frequency (n)</td><td>Percent (%)</td></tr><tr><td colspan="3">Childhood vaccines are essential for a child's health</td></tr><tr><td>Strongly agree</td><td>169</td><td>40.1</td></tr><tr><td>Agree</td><td>128</td><td>30.3</td></tr><tr><td>Neither agree nor disagree</td><td>63</td><td>14.9</td></tr><tr><td>Disagree</td><td>24</td><td>5.7</td></tr><tr><td>Strongly disagree</td><td>38</td><td>9.0</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td colspan="3">Getting vaccines is a good way to protect children from diseases</td></tr><tr><td>Strongly agree</td><td>217</td><td>51.4</td></tr><tr><td>Agree</td><td>112</td><td>26.5</td></tr><tr><td>Neither agree nor disagree</td><td>36</td><td>8.5</td></tr><tr><td>Disagree</td><td>34</td><td>8.1</td></tr><tr><td>Strongly disagree</td><td>23</td><td>5.5</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td colspan="3">Measles vaccine is received at nine months</td></tr><tr><td>Strongly agree</td><td>178</td><td>42.3</td></tr><tr><td>Agree</td><td>66</td><td>15.6</td></tr><tr><td>Neither agree nor disagree</td><td>18</td><td>4.3</td></tr><tr><td>Disagree</td><td>104</td><td>24.6</td></tr><tr><td>Strongly disagree</td><td>56</td><td>13.2</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td colspan="3">The vaccination schedule should be completed within twelve months</td></tr><tr><td>Strongly agree</td><td>76</td><td>18.0</td></tr><tr><td>Agree</td><td>58</td><td>13.7</td></tr><tr><td>Neither agree nor disagree</td><td>161</td><td>38.2</td></tr><tr><td>Disagree</td><td>56</td><td>13.3</td></tr><tr><td>Strongly disagree</td><td>71</td><td>16.8</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">Oral polio should be received three times</td></tr><tr><td>Strongly agree</td><td>15</td><td>3.6</td></tr><tr><td>Agree</td><td>33</td><td>7.8</td></tr><tr><td>Neither agree nor disagree</td><td>224</td><td>53.1</td></tr><tr><td>Disagree</td><td>52</td><td>12.3</td></tr><tr><td>Strongly disagree</td><td>98</td><td>23.2</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr></table>
## ii. Summary of Participant's Perceptions towards Child Vaccination
Most respondent's perceptions were assessed regarding child vaccination. Specific perceptions are classified into six classes: (i) many communities and caregivers reject routine immunization due to rumors, incorrect information, and fear; (ii) lack of confidence and trust in routine immunization as effective health interventions appear to be relatively common in all parts of Nigeria; (iii) routine immunization is to depopulate the community; (iv) routine immunization will make children impotent when they grow up; (v) afraid that child/children will be infected with a virus; and (vi) it is not a crime in my religion to be vaccinated (see Table 5). They are categorized by frequency in the included works, regarded below as 'n'. In conclusion, the most regularly stated perceptions consisted of many communities and caregivers reject routine immunization due to rumors, incorrect information, and fear (n = 269, $53.8\%$ ); lack of confidence and trust in routine immunization as effective health interventions appears to be relatively common in all parts of Nigeria (n = 216, $51.2\%$ ); routine immunization is to depopulate the community ( $n = 213$, $50.4\%$ ); routine immunization will make children impotent when they grow up ( $n = 264$, $62.6\%$ ); afraid that child/children will be infected with a virus ( $n = 193$, $45.8\%$ ); and it is not a crime in my religion to be vaccinated ( $n = 298$, $70.6\%$ ). Generally, perception was evaluated with the composite immunization perception score of participants, which signified $30.6\%$ for good perception and $69.4\%$ for poor perception concerning immunization. Good perception was obtained more among participants in Ibadan South East ( $39.9\%$ ) likened to Ibadan North ( $19.6\%$ ) as displayed in Figure 8.
Table 5: Summary of Participant's Perceptions towards Child Vaccination
<table><tr><td>Variables</td><td>Frequency (n)</td><td>Percentage (%)</td></tr><tr><td>Many communities and caregivers reject routine immunization due to rumors, incorrect information, and fear</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>154</td><td>36.5</td></tr><tr><td>Agree</td><td>115</td><td>27.3</td></tr><tr><td>Neither agree nor disagree</td><td>54</td><td>12.8</td></tr><tr><td>Disagree</td><td>43</td><td>10.2</td></tr><tr><td>Strongly disagree</td><td>56</td><td>13.2</td></tr><tr><td>Total</td><td>422</td><td>100.0</td></tr><tr><td>Lack of confidence and trust in routine immunization as effective health intervention appears to be relatively common in all parts of Nigeria</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>113</td><td>26.8</td></tr><tr><td>Agree</td><td>103</td><td>24.4</td></tr><tr><td>Neither agree nor disagree</td><td>59</td><td>13.9</td></tr><tr><td>Disagree</td><td>78</td><td>18.5</td></tr><tr><td>Strongly disagree</td><td>69</td><td>16.4</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td>Routine immunization is to depopulate the community</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>62</td><td>14.7</td></tr><tr><td>Agree</td><td>53</td><td>12.6</td></tr><tr><td>Neither agree nor disagree</td><td>94</td><td>22.3</td></tr><tr><td>Disagree</td><td>112</td><td>26.5</td></tr><tr><td>Strongly disagree</td><td>101</td><td>23.9</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td>Routine immunization will make children impotent when they grow up</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>61</td><td>14.4</td></tr><tr><td>Agree</td><td>40</td><td>9.5</td></tr><tr><td>Neither agree nor disagree</td><td>57</td><td>13.5</td></tr><tr><td>Disagree</td><td>121</td><td>28.7</td></tr><tr><td>Strongly disagree</td><td>143</td><td>33.9</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td>Afraid that child/children will be infected with a virus</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>77</td><td>18.3</td></tr><tr><td>Agree</td><td>58</td><td>13.7</td></tr><tr><td>Neither agree nor disagree</td><td>94</td><td>22.2</td></tr><tr><td>Disagree</td><td>110</td><td>26.1</td></tr><tr><td>Strongly disagree</td><td>83</td><td>19.7</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td>It is not a crime in my religion to be vaccinated</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>144</td><td>34.1</td></tr><tr><td>Agree</td><td>154</td><td>36.5</td></tr><tr><td>Neither agree nor disagree</td><td>8</td><td>1.9</td></tr><tr><td>Disagree</td><td>94</td><td>22.3</td></tr><tr><td>Strongly disagree</td><td>22</td><td>5.2</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr></table>
## iii. Summary of Participant's Perceived Barriers to Child Vaccination
Most participants perceived barriers to child vaccination. Specific perceived barriers are classified into nine subtitles: (i) health staff who deal with mothers in an unfavorable, rude, and sometimes abusive manner were found to be associated with the mother's refusal for bringing children for vaccination; (ii) health workers shouting at mothers who forgot to bring their children's immunization record cards or missed scheduled appointments affects the completion of RI services; (iii) behaviour of healthcare workers could undermine trust in the health workers and could also discourage caregivers from listening to health education messages; (iv) healthcare workers with calm and friendly attitude towards caregivers increases respond to vaccination information during RI session; (v) lack of confidence in healthcare workers made me not complete my child's immunization; (vi) lack of vehicular movement hinders my child immunization; (vii) mothers that are domiciled near a health facility providing RI services are more likely to fully immunize their children than those living in areas where there are no health facilities providing RI close to them; (viii) long walking distances, as well as long waiting time at the facility, are critical factors associated with poor completion of RI schedules; and (ix) lack of good roads to health centre affected my child's immunization completion (see Table 6). Perceived barriers for non-vaccination of mothers/caregivers of children aged 9 to 12 months who were not or partially vaccinated in the Ibadan North and Ibadan South East health district in 2022. Four hundred and twenty-two mothers/caregivers of children aged 9 to 12 months who were not or partially vaccinated gave the reasons for not vaccinating their child. Health staff who deal with mothers in an unfavorable, rude, and sometimes abusive manner (n = 368, 87.2%); health workers shouting at mothers who forgot to bring their children's immunization record cards or missed scheduled appointments affects the completion of RI services (n= 337, 79.8%); behaviour of healthcare workers could undermine trust in the health workers and could also discourage caregivers from listening to health education messages (n= 335, 79.3%); healthcare workers with
calm and friendly attitude towards caregivers increases respond to vaccination information during RI session (n=345, 77.7%); lack of confidence in HCWs made me not complete my child's immunization (n=299, 70.8%); lack of vehicular movement hinders my child immunization (n=292, 69.2%); mothers that are domiciled near a health facility providing RI services are more likely to fully immunize their children than those living in areas where there are no health facilities providing RI close to them (n= 333, 78.9%); long walking distances, as well as long waiting time at the facility, are critical factors associated with poor completion of RI schedules (n= 334, 78.1%); and lack of good roads to health centre affected my child's immunization completion (n= 325, 77.0%) were the nine reasons most frequently mentioned.
Table 6: Summary of Participant's Perceived Barriers to Child Vaccination
<table><tr><td>Variables</td><td>Frequency (n)</td><td>Percent (%)</td></tr><tr><td colspan="3">Health staff who deal with mothers in an unfavorable, rude, and sometimes abusive manner were found to be associated with the mother's refusal to bring children for vaccination.</td></tr><tr><td>Strongly agree</td><td>197</td><td>46.7</td></tr><tr><td>Agree</td><td>171</td><td>40.5</td></tr><tr><td>Neither agree nor disagree</td><td>3</td><td>0.7</td></tr><tr><td>Disagree</td><td>31</td><td>7.4</td></tr><tr><td>Strongly disagree</td><td>20</td><td>4.7</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">Health workers screaming at mothers who forgot to bring their children's immunization record cards or missed scheduled appointments affect the completion of RI services</td></tr><tr><td>Strongly agree</td><td>162</td><td>38.4</td></tr><tr><td>Agree</td><td>175</td><td>41.4</td></tr><tr><td>Neither agree nor disagree</td><td>8</td><td>1.9</td></tr><tr><td>Disagree</td><td>65</td><td>15.5</td></tr><tr><td>Strongly disagree</td><td>12</td><td>2.8</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">Behaviour of healthcare workers could undermine trust in the health workers and could also discourage caregivers from listening to health education messages.</td></tr><tr><td>Strongly agree</td><td>195</td><td>46.2</td></tr><tr><td>Agree</td><td>140</td><td>33.1</td></tr><tr><td>Neither agree nor disagree</td><td>8</td><td>1.9</td></tr><tr><td>Disagree</td><td>59</td><td>14.0</td></tr><tr><td>Strongly disagree</td><td>20</td><td>2.8</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">HCWs with calm and friendly attitudes towards caregivers increase response to vaccination information during RI sessions.</td></tr><tr><td>Strongly agree</td><td>186</td><td>40.0</td></tr><tr><td>Agree</td><td>159</td><td>37.7</td></tr><tr><td>Neither agree nor disagree</td><td>2</td><td>0.5</td></tr><tr><td>Disagree</td><td>56</td><td>13.3</td></tr><tr><td>Strongly disagree</td><td>19</td><td>4.5</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td colspan="3">Lack of confidence in healthcare workers made me not complete my child's immunization.</td></tr><tr><td>Strongly agree</td><td>176</td><td>41.7</td></tr><tr><td>Agree</td><td>123</td><td>29.1</td></tr><tr><td>Neither agree nor disagree</td><td>11</td><td>2.6</td></tr><tr><td>Disagree</td><td>94</td><td>22.3</td></tr><tr><td>Strongly disagree</td><td>18</td><td>4.3</td></tr><tr><td>Lack of vehicular movement hinders my child's immunization</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>147</td><td>34.8</td></tr><tr><td>Agree</td><td>145</td><td>34.4</td></tr><tr><td>Neither agree nor disagree</td><td>11</td><td>2.6</td></tr><tr><td>Disagree</td><td>95</td><td>22.5</td></tr><tr><td>Strongly disagree</td><td>24</td><td>5.7</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td>Mothers who are domiciled near a health facility providing RI services are more likely to fully immunize their children than those living in areas where there are no health facilities are providing RI close to them.</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>187</td><td>44.3</td></tr><tr><td>Agree</td><td>146</td><td>34.6</td></tr><tr><td>Neither agree nor disagree</td><td>12</td><td>2.8</td></tr><tr><td>Disagree</td><td>59</td><td>13.9</td></tr><tr><td>Strongly disagree</td><td>18</td><td>4.4</td></tr><tr><td>Long walking distances, as well as long waiting times at the facility, are critical factors associated with poor completion of RI schedules</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>158</td><td>37.4</td></tr><tr><td>Agree</td><td>176</td><td>41.7</td></tr><tr><td>Neither agree nor disagree</td><td>14</td><td>3.3</td></tr><tr><td>Disagree</td><td>61</td><td>14.5</td></tr><tr><td>Strongly disagree</td><td>13</td><td>3.1</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr><tr><td>The lack of good roads to the health center affected my child's immunization completion</td><td></td><td></td></tr><tr><td>Strongly agree</td><td>196</td><td>46.4</td></tr><tr><td>Agree</td><td>129</td><td>30.6</td></tr><tr><td>Neither agree nor disagree</td><td>13</td><td>3.1</td></tr><tr><td>Disagree</td><td>68</td><td>16.1</td></tr><tr><td>Strongly disagree</td><td>16</td><td>3.8</td></tr><tr><td>Total</td><td>422</td><td>100</td></tr></table>
iv. Summary of Associated Factors with Child Immunization Coverage in Ibadan North and South East Primary Healthcare Centers
Associated factors with child immunization coverage in 9-12 months children are classified into ten subheadings: (i) knowledge of vaccination; (ii) perception of child vaccination; (iii) LGA; (iv) age category; (v) occupation; (vi) number of children; (vii) marital status; (viii) academic status; (ix) monthly income; and (x) religion (see Table 7). They are categorized by frequency of inclusion in the works investigated, regarded as 'n' (see also Table 7). In short, the most often determinant factors for estimating child immunization coverage utilizing Chi-square were: knowledge of vaccination (23.544), perception of child vaccination (27.528), LGA (1.293), age category (4.034), occupation (27.318), number of children (8.316), marital status (7.734), educational qualification (27.318), monthly income (20.521); and religion factors (1.091).
Multivariable regression analysis to model employing the probability ratio technique (forward: LR) was used to estimate the share of association between vaccination knowledge, perception, and socio-demographic factors in the prediction of the complete vaccination among children while controlling for the confounders. This analysis revealed that knowledge of vaccination was the significant predictors of vaccination coverage. Among these three variables (e.g., knowledge, perception, and socio-demographic factors), the level of knowledge was the most influential factor in this respect (AOR: 0.34, CI: 0.19 - 0.58, p<0.001), followed by the level of perception (AOR: 0.28, CI: 0.16 - 0.47, p<0.001). Generally, the likelihoods of exposure to complete immunization coverage were 0.34 and 0.28, respectively (see Table7).
Table 7: Summary of Associated Factors with Child Immunization Coverage using Chi- Square
<table><tr><td rowspan="2">Factors</td><td colspan="2">Received less than five vaccines at nine months and above</td><td colspan="2">Received all five vaccines at nine months and above</td><td rowspan="2">Total</td><td rowspan="2">X2</td><td rowspan="2">P</td></tr><tr><td>N</td><td>%</td><td>N</td><td>%</td></tr><tr><td>Knowledge of Vaccination</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Low knowledge</td><td>175</td><td>70.3</td><td>74</td><td>29.7</td><td>249</td><td>23.544</td><td>0.000</td></tr><tr><td>High knowledge</td><td>81</td><td>46.8</td><td>92</td><td>53.2</td><td>173</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr><tr><td>Perception of child vaccination</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Poor perception</td><td>202</td><td>68.9</td><td>91</td><td>31.1</td><td>293</td><td>27.528</td><td>0.000</td></tr><tr><td>Good perception</td><td>54</td><td>41.9</td><td>75</td><td>58.1</td><td>129</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr><tr><td>LGA</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Ibadan North</td><td>112</td><td>57.7</td><td>82</td><td>42.3</td><td>194</td><td>1.293</td><td>0.255</td></tr><tr><td>Ibadan South East</td><td>144</td><td>63.2</td><td>84</td><td>36.8</td><td>228</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr><tr><td>Age category</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>14 to 18 years</td><td>8</td><td>72.7</td><td>3</td><td>27.3</td><td>11</td><td>4.034</td><td>0.401</td></tr><tr><td>19 to 23 years</td><td>28</td><td>65.1</td><td>15</td><td>34.9</td><td>43</td><td></td><td></td></tr><tr><td>24 to 28 years</td><td>88</td><td>55.0</td><td>72</td><td>45.0</td><td>160</td><td></td><td></td></tr><tr><td>29 to 33 years</td><td>70</td><td>64.8</td><td>38</td><td>35.2</td><td>108</td><td></td><td></td></tr><tr><td>34 years and above</td><td>62</td><td>62.0</td><td>38</td><td>38.0</td><td>100</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr><tr><td>Occupation</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Housewife</td><td>41</td><td>62.1</td><td>25</td><td>37.9</td><td>66</td><td>27.318</td><td>0.000</td></tr><tr><td>Trader</td><td>144</td><td>70.9</td><td>59</td><td>29.1</td><td>203</td><td></td><td></td></tr><tr><td>Artisan</td><td>13</td><td>37.1</td><td>22</td><td>62.9</td><td>35</td><td></td><td></td></tr><tr><td>Skilled worker</td><td>27</td><td>50.9</td><td>26</td><td>49.1</td><td>53</td><td></td><td></td></tr><tr><td>Civil servant</td><td>26</td><td>44.1</td><td>33</td><td>55.9</td><td>59</td><td></td><td></td></tr><tr><td>Other, specify</td><td>2</td><td>100.0</td><td>0</td><td>0.0</td><td>2</td><td></td><td></td></tr><tr><td>Total</td><td>253</td><td>60.5</td><td>165</td><td>39.5</td><td>418</td><td></td><td></td></tr><tr><td>Number of children</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>1-2 children</td><td>75</td><td>51.4</td><td>71</td><td>48.6</td><td>146</td><td>8.316</td><td>0.000</td></tr><tr><td>3-4 Children</td><td>160</td><td>66.1</td><td>82</td><td>33.9</td><td>242</td><td></td><td></td></tr><tr><td>Five or more children</td><td>21</td><td>61.8</td><td>13</td><td>38.2</td><td>34</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr><tr><td>Marital Status</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Single</td><td>1</td><td>16.7</td><td>5</td><td>83.3</td><td>6</td><td>7.734</td><td>0.052</td></tr><tr><td>Married</td><td>250</td><td>61.4</td><td>157</td><td>38.6</td><td>407</td><td></td><td></td></tr><tr><td>Cohabiting</td><td>1</td><td>100.0</td><td>0</td><td>0.0</td><td>1</td><td></td><td></td></tr><tr><td>Widowed/separated</td><td>1</td><td>25.0</td><td>3</td><td>75.0</td><td>4</td><td></td><td></td></tr><tr><td>Total</td><td>253</td><td>60.5</td><td>165</td><td>39.5</td><td>418</td><td></td><td></td></tr><tr><td>Educational Qualification</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>No formal education</td><td>22</td><td>81.5</td><td>5</td><td>18.5</td><td>27</td><td>27.318</td><td>0.000</td></tr><tr><td>Primary education</td><td>71</td><td>76.3</td><td>22</td><td>23.7</td><td>93</td><td></td><td></td></tr><tr><td>Secondary education</td><td>77</td><td>63.1</td><td>45</td><td>36.9</td><td>122</td><td></td><td></td></tr><tr><td>Higher education</td><td>86</td><td>47.8</td><td>94</td><td>52.2</td><td>87</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr><tr><td>Factors</td><td colspan="2">Received less than five vaccines at nine months and above</td><td colspan="2">Received all five vaccines at nine months above</td><td>Total</td><td>X2</td><td>P</td></tr><tr><td>Monthly Income</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>0 - 18,0000</td><td>121</td><td>69.9</td><td>52</td><td>30.1</td><td>173</td><td>20.521</td><td>0.000</td></tr><tr><td>18,000-40,000</td><td>57</td><td>45.2</td><td>69</td><td>54.8</td><td>126</td><td></td><td></td></tr><tr><td>41,000-60,000</td><td>31</td><td>59.6</td><td>21</td><td>40.4</td><td>52</td><td></td><td></td></tr><tr><td>61,000-80,000</td><td>20</td><td>60.6</td><td>13</td><td>39.4</td><td>33</td><td></td><td></td></tr><tr><td>81,000 and above</td><td>25</td><td>71.4</td><td>10</td><td>28.6</td><td>35</td><td></td><td></td></tr><tr><td>Total</td><td>254</td><td>60.6</td><td>165</td><td>39.4</td><td>419</td><td></td><td></td></tr><tr><td>Religion</td><td></td><td></td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Christianity</td><td>101</td><td>58.0</td><td>73</td><td>42.0</td><td>174</td><td>1.091</td><td>0.580</td></tr><tr><td>Islam</td><td>150</td><td>62.2</td><td>91</td><td>37.8</td><td>241</td><td></td><td></td></tr><tr><td>Others</td><td>5</td><td>71.4</td><td>2</td><td>28.6</td><td>7</td><td></td><td></td></tr><tr><td>Total</td><td>256</td><td>60.7</td><td>166</td><td>39.3</td><td>422</td><td></td><td></td></tr></table>
## IV. DISCUSSION OF FINDINGS
By result of this work, the status of immunization coverage varies in both Local Government Areas and vaccine. Coverage of many vaccines were high while few were low. The pentavalent vaccine had the maximum (79%) overall mean coverage in both Ibadan North (92%) and Ibadan South East (66%). Polio immunization coverage comes next to that of pentavalent with overall mean coverage rate (77.7%) in Ibadan North (92.3%) and Ibadan Southeast (65.4%), respectively. Pneumonia had an overall vaccine rate (68.3%) with Ibadan North (87%) and Ibadan South East (49.6%). Measles overall vaccination rate (62.3%) with Ibadan North had (59.3%) and Ibadan South East (64.9%). Yellow fever overall injection rate (59%) with Ibadan North (59%) and Ibadan South East (60%), respectively. It is clear from the finding of study that pentavalent, polio, pneumonia, measles, and yellow-fever vaccine had coverage rate that were above average in both LGAs. Notwithstanding, the coverage of pentavalent, polio, and pneumonia vaccines were more in Ibadan North relative to Ibadan South East, while measles injection rate was more remarkable in Ibadan South East than Ibadan North and the rate is just at the same range for yellow-fever in both LGAs. The immunization status in Ibadan North and Ibadan South East were poor likened to the result in a survey carried out in Osun State Nigeria that detected 80% coverage rate for all antigens administered at birth. These vaccines (BCG, OPV0, and HBV1) had greater coverage levels (Adedire et al., 2016).
Furthermore, results signified that the percentage of missed vaccination was lower in Ibadan North (14%) with Ibadan South East (43.9%) and primary reason for missed vaccination is child sickness, the rest reasons indicated were no vaccine at the clinic and long waiting time at the health center. The work obtained complete immunization coverage for all five vaccines at
39.3%. The status of immunization coverage in this work is likewise related to Ibadan North East and Ido by Fatiregun et al. (2013), which revealed that the weighted complete injection coverage was $40.2\%$ and $41.3\%$ in Ibadan North East and Ido, respectively.
Our results showed that awareness and knowledge of vaccines among mothers/caregiver were high, more significant part (70%) of participants were conscious that childhood vaccines were crucial for the child and significant percentage (78%) expressed that receiving vaccines for their child is a best method to immune the child from illnesses. Notwithstanding, caregivers understanding on particular immunization information like vaccination date for all injections were not very sufficient because more significant part of them counts on records on vaccination cards and database offered by health personnel.
About perception, just $39.9\%$ of sampled caregivers in Ibadan South East had good perception concerning immunization and few $(19.6\%)$ had good perception toward immunization in Ibadan North. More significant part of the sampled respondents are still of the notion that vaccination may be utilized to depopulate the society and children may become infertile or affected with virus. The result of this analysis is related to the deduction of Fatiregun et al. (2013) result that shows that non-completion of immunization or non-immunization is mostly be as a result of unawareness regarding injection schedule and fear of aftermaths of vaccination.
Hints on factors associated with poor immunization coverage indicate that more significant part (64%) of caregivers assumed that rumors of aftermaths, inadequate information, and fear inhibit complete immunization coverage in both Ibadan North and Ibadan South East. The rest indicated factors resulting in mothers rebuff to bring children for vaccination are related to negative attitude of health personnel. For health officer attitude causing hindrance to complete immunization program, this work is not the just work that detects the attitude and conduct of health officers as hindrance to immunization coverage. The study by Rahji and Ndikom (2013), determined in Ibadan too concur that health providers' attitude is a factor hinders conformity with vaccination schedules. Most mother/caregivers may find it hard to relate sufficiently with some health officers and this poor relational association may deter the immunization completion.
Our results also revealed that caregivers' understanding of vaccination, perception concerning vaccination, and the socio-demographic, for example, academic status, mothers' profession, and earnings, are all related to complete immunization in children. Mothers/caregivers who have a good knowledge of vaccination had significantly higher proportion of their children who acquired all five vaccines. Also, mothers/caregivers with poor perception of child vaccination had a reduced percentage of their children obtaining all five vaccinations. Other factors that indicated statistical significance with vaccination coverage were work, parity, academic status, and earnings. Nevertheless, age of the mothers/caregivers was not statistically associated with immunization coverage rate. This result is in harmony with the result in Bungudu, Zamfara State, North West Nigeria (Adedokun et al., 2017), signified that degree of knowledge on RI and obtaining at a minimum secondary school is considerably related to complete immunization. Likewise, this study is in agreement with the Abdulraheem et al. (2020) finding that indicates that there is no statistical differences about immunization fullness as a result of determinants like marital level, age of mothers', and sex of the child. Thus, the results of this work and previous literature affirmed the reality that the academic status of the mother/caregiver is more crucial to immunization coverage than the rest of demographic factors like age or marital level; this could be a result of the truth that there is no age that is most likely be excessive or inadequate for dissemination of information, any person at any age class or marital level could fathom and use any medical associated information specified by health workers.
Moreover, Shelton et al. (2013) deduced in their work that the profession of mothers/caregivers can deter the completion of immunization in children. Occupation schedule particularly in public servants are continuously hard to change, so mothers who fall under this group of labor force who usually resume at 8 in the morning which is the similar time appoint for most immunization appointment may find it hard to attend all injection schedules. Likewise, result from this work is in harmony with the Ethiopian research which ascribed unawareness concerning immunization to poor coverage. The work too asserted that children of mothers that understood the age in which vaccination needs to begin and finishes have the probability to finish vaccination appointment likened to those whose mothers are uneducated of RI appointment (Shelton et al., 2013).
## V. CONCLUSION
Immunization is directed at the averting of infectious diseases and it is a crucial community medical intervention and a cost-efficient approach to decline fatality and morbidity related to infectious diseases. Complete immunization coverage for all the five vaccines in Ibadan North and Ibadan South East is low relative to the WHO guideline limit. Notwithstanding, a few critical child vaccine like pentavalent, polio, pneumonia, measles, and yellow-fever vaccine had coverage level that were more than average in both LGAs. Causes for missed vaccination were child sickness, lack of vaccine at the health center, long waiting time at the medical building, and poor attitude of health personnel. Conscious and understanding of vaccines among caregivers in both Ibadan North and Ibadan South East were high and knowledge of childhood vaccines were crucial to adequate vaccination of children. Mothers/caregivers' understanding of vaccination, perception regarding immunization and the socio-demographic like academic qualification, mothers' profession, and earnings were all related to complete vaccination in children. Mothers/caregivers who have good knowledge on immunization had considerably more significant proportion of their children who had all five vaccines. Similarly, mothers/caregivers with low perception of child immunization have a reduced proportion of their children getting all five vaccinations. Other factors that demonstrated statistical differences with immunization coverage are profession, parity, academic level, and earnings. Nevertheless, age of mothers/caregiver was not significantly associated with vaccination coverage status. This study recommended that health officers and health educators need to stress the significance of immunization and also attempt to decry all the wrong beliefs and negative attitudes on immunization.
## VI. LIMITATION OF THE STUDY
The following are limitations to the work:
1. Participants Potential Social Desirability, bias among participants, and the truth that causality from a cross sectional study cannot be determined and there is limitation to potential generalization of results.
2. Participants Attitude: Because of the nature of technique of gathering data (Kobo Collect) which is unpopular not like printed questionnaire, the participants felt hesitant to answers the question willingly as anticipated but with compelling clarification and education, they thereafter concurred.
### ACKNOWLEDGEMENTS
3. COVID-19 Pandemic Associated Factors: The pandemic which has led to a new rule of wearing masks and physical distancing hindered the participants to willingly relate but after several episodes of data gathering they conformed.
- This study is taken from a MSc dissertation of Community Health approved by the Research Ethics Review Committee of Department of Planning, Research, and Statistics Division, Ministry of Health, Oyo State, Nigeria (code number: AD 13/479/4307A). The authors express their thanks for the cooperation and assistance of the authorities of the Department of Public Health, Faculty of Basic and Medical Science, Lead City University, Ibadan, and all the organizations and people who assisted us in this work. We also thank health officials and members of Health Committees of Ibadan North and South East Health Districts for facilitating this work. The authors are also grateful to the anonymous reviewers for their enlightening, constructive, and helpful comments on the paper.
- Statement of Competing Interests
- The author(s) declared no potential conflicts of interest in terms of the research, authorship, and/or publication of this manuscript.
- Funding
- The author(s) received no financial support for the research, authorship, and/or publication of this paper.
- Abbreviations:
- EPI: Expanded Program on Immunization;
- GAVI: Global Alliance for Vaccines and Immunization; WHO: World Health Organization;
- DTP: diphtheria, tetanus, and pertussis vaccine;
- HDI: Human Development Index;
- USA: United States of America;
- PHC: Primary Health Care service;
- RI: Routine immunization; HCWs: healthcare workers
Generating HTML Viewer...
References
13 Cites in Article
I Abdulraheem,A Onajole,A Jimoh,A Oladipo (2011). Reasons for incomplete vaccination and factors for missed opportunities among rural Nigerian children.
Sulaimon Adedokun,Olalekan Uthman,Victor Adekanmbi,Charles Wiysonge (2017). Incomplete childhood immunization in Nigeria: a multilevel analysis of individual and contextual factors.
Feilden Analysts,Battersby (2005). Design of routine immunization initiative-Trip report for DFID.
V Ankrah,F Nwaigwe (2005). Immunization system review and training needs assessment in Ekiti State.
Belachew Etana,Wakgari Deressa (2012). Factors associated with complete immunization coverage in children aged 12–23 months in Ambo Woreda, Central Ethiopia.
A Fatiregun,A Adebowale,R Ayoka,A Fagbamigbe (2013). Assessing full immunisation coverage using lot quality assurance sampling in urban and rural districts of southwest Nigeria.
Akinola Fatiregun,Ayo Adebowale,Rita Ayoka,Adeniyi Fagbamigbe (2013). Assessing full immunisation coverage using lot quality assurance sampling in urban and rural districts of southwest Nigeria.
Anthony Fiore,Carolyn Bridges,Nancy Cox (2019). Seasonal Influenza Vaccines.
Karen Glanz,Donald Bishop (2010). The Role of Behavioral Science Theory in Development and Implementation of Public Health Interventions.
Holly Hill,David Yankey,Laurie Elam-Evans,James Singleton,Natalie Sterrett (2021). Vaccination Coverage by Age 24 Months Among Children Born in 2017 and 2018-National Immunization Survey-Child, United States, 2018-2020.
Ibidolapo Ijarotimi,Akinola Fatiregun,Adebiyi,A Oluwapelumi,Olayinka Ilesanmi,Ajumobi,Olalekan Olufemi; Uthman (2018). Urban-rural differences in immunisation status and associated demographic factors among children 12-59 months in a southwestern state, Nigeria.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Taiwo O. Ogunwale. 2026. \u201cAssessment of Levels of Immunization and Factors Associated with the Non-completion Routine Immunization within (9-12 Months) Attending Primary Healthcare Centres in Ibadan North and South East, Nigeria\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 25 (GJMR Volume 25 Issue K2): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Immunization is designed to prevent transmittable diseases and it is an integral public medical intervention and an economical method to decline mortality and morbidity associated with transmittable diseases. This work attempts to determine the vaccine coverage and factors related to the non-completion routine immunization within babies (9-12 months) attending Primary Healthcare Centre (PHC) in Ibadan North and South East Local Government Areas, Oyo State.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Assessment of Levels of Immunization and Factors Associated with the Non-completion Routine Immunization within (9-12 Months) Attending Primary Healthcare Centres in Ibadan North and South East, Nigeria




































































