### 1. INTRODUCTION
Noises related to the firing of a weapon derive from three sources:
1. Noises produced by the firing and ejection mechanism of the weapon;
2. Noises produced by the firing gas expansion of the weapon;
3. Noises produced by the projectile in the air and at the moment of impact.
With regard to the first point, in ordinary repeating weapons there is only the noise of the trigger pull and the firing pin striking the primer; in automatic weapons there may be the noise of the beating mass striking, retroceding and recambering a cartridge [1]. Such noises are almost always masked by the sounds of the actual firing and assume some prominence only in weapons equipped with silencers [2].
The actual firing, on the other hand, is produced by the rapid expansion of gases that exit the muzzle of the weapon with a velocity that can be twice that of the projectile and with a pressure of several hundred atmospheres [3, 4]. Three basic components can be distinguished in shot noise.
a) the precursor wave, caused by the fact that the bullet, as it travels through the barrel, accelerates and compresses the air in it, so that the bullet is preceded by a wave that reaches a pressure of several atmospheres. This wave may cumulate with that caused by those gases which, by defect of adherence between the barrel and the projectile, manage to overcome and precede the projectile.
b) the wave caused by the sudden displacement of the air mass at the muzzle of the weapon when the projectile exits from it; it is normally negligible, but assumes importance in silenced weapons;
c) the wave caused by the exit of hot gases from the blast (muzzle blast), constituting the dominant noise in nonsilenced weapons, which lasts less than 3
milliseconds [5]. The pressure of this wave depends basically on the gas pressure and this, in turn, on the length of the barrel and the type of powder. Short barrels and progressive powders result in high muzzle pressures; the opposite is true with long barrels or lively powders. A short barrel in relation to the burning rate of the powder produces a considerable increase in the intensity of firing, although it does not necessarily increase the gas pressure, since it may be the case that unburned gases come out of the barrel which, combining with the oxygen in the air, explode thunderously (muzzle fire).
There are three noises produced by the bullet during its flight:
a) The first noise is the hissing sound. It can be attributed to both vortices and the suction of air behind the projectile.
b) The second noise, analogous to the sound of the projectile bouncing back after hitting an obstacle, takes over under certain circumstances and is the buzzing noise produced by the poorly stabilized non-spherical projectile. As is well known, the rifling of the barrel imparts a very rapid rotational motion to the projectile, which can be as high as 3,000 revolutions per second. Stabilization of the bullet is never perfect, and some causes of destabilization can be a defect in the muzzle of the weapon, hitting against obstacles, crossing a liquid or solid body, etc...
c) The third sound, called ballistic wave (sonic crack), is that produced by a projectile traveling at supersonic speed (more than $330~\mathrm{m / sec}$ ). It is nothing more than the effect of the explosive wave of gas from the launching charge, which, suddenly releasing itself into the air at a speed greater than the speed of sound, causes a violent change in air pressure, which propagates not only forward from the muzzle of the weapon, but also in every other direction. The intensity of the ballistic wave is about 136-140 dB.
The sound spreads through the air in the form of concentric pressure waves. A projectile, which in its
flight must overcome the resistance of the air layers and by its motion continuously presses ahead of itself, produces pressure pulses that spread through the air with relative speed equal to that of sound, but which will also be subject to being carried by the air current in the opposite direction to that of the projectile and with equal speed. This effect is confined in a cone, called the Mach
cone) (Figures 1) whose vertex is the projectile and whose opening angle decreases from $180^{\circ}$ to gradually smaller values as the velocity increases. The Mach cone separates the zone of silence, outside it, from the zone inside it where the noise is concentrated. The noise (so-called bang) is perceived by our ear only when it is hit by the front of the cone [6].
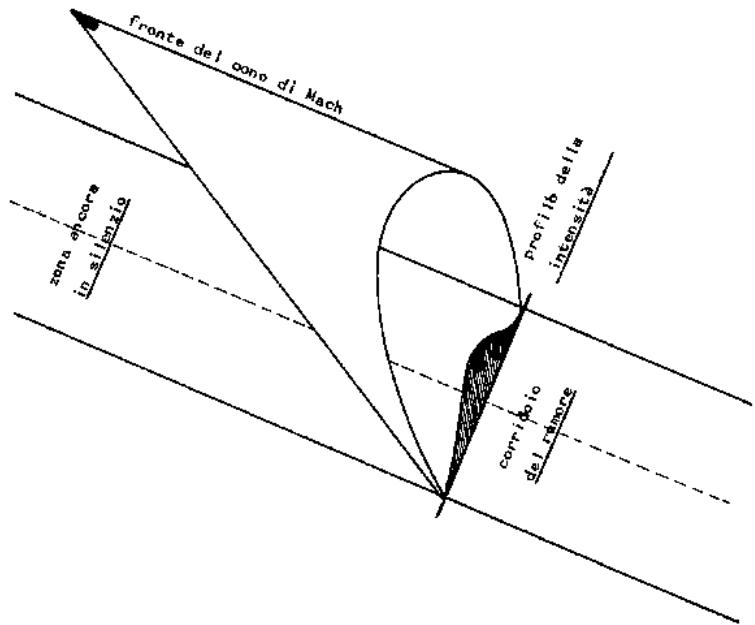
Fig. 1
In addition, the intensity of sound is inversely proportional to the distance from the sound source, that is, it decreases as one moves away from it and varies in inverse proportion to the square of the distance: with each doubling of the distance there is a decrease of 6 dB.
It must then be taken into account that different conditions of the atmosphere passed through contribute to the attenuation. There are no precise data on attenuation due to rain, fog, or falling snow; it is generally accepted to be around 15 dB per kilometer. When sound spreads close to the ground there is also absorption by vegetation, which on soils with grass and bushes is around 0.1 dB per meter. The propagation of sound through rocks and soil is typically at least 5 times faster than the speed of sound through air. Due to temperature effects, the speed of sound varies in different atmospheric layers and sound waves are deflected upward or downward [7, 8].
As far as wind is concerned, what happens is that the speed of the wind and the speed of sound add up vectorially, and as wind speed decreases as it approaches the ground, it happens that sounds following the same direction as the wind are deflected toward the ground and those against the wind are deflected upward.
The presence of obstacles along the projectile's trajectory can cause reverberation (reflection of the sound wave by an obstacle placed in front of the sound
source) and diffraction (a phenomenon associated with the deviation of the propagation trajectory of sound waves when they encounter an obstacle in their path), which can alter the intensity of sound.
### a) Silencer
A silencer is a suppressor or moderator of sound in firearms. Silencing of firing is required in military and civilian leaders for several reasons:
- prevent immediate and accurate detection of the direction and distance from which the shot starts;
- not to alarm the opponent;
- reduce the flare, i.e., the emission of light (and fumes) and thus make the shooter less visible in low-light conditions;
- the shooter is not subject to the physical shock of firing.
The silencer can only attenuate the noise produced by the muzzle wave; on the other hand, it cannot affect in any way the noise produced by the weapon mechanism or the bullet, much less the noise of the ballistic wave. It is for this reason that in all silenced weapons employing ammunition developing supersonic velocity, an attempt is made to reduce the initial velocity of the projectile to subsonic velocity either by employing ammunition with suitably reduced launching charge, oppose by modifying the barrel of the weapon with firing
gas intakes, which cause a decrease in pressure and consequently in velocity.
The systems devised so far to attenuate the muzzle wave all seek to subtract energy from the firing gases in various ways. The systems applied, singly or jointly are expansion of the gases in a container, absorption of heat by lamellar radiators, metal filaments, liquids, and the silencer walls themselves, formation of turbulence inside the silencer (to slow down the velocity of the gases), transformation into work of the energy of the gases, which must compress springs to escape.
In essence, a gun silencer is quite similar to a silencer for internal combustion engines, the only difference being that the former must be drilled so as to allow the bullet to pass through, which prevents total noise attenuation (this could be achieved only with practically unacceptable silencer dimensions). In some silencers the hole for the bullet is closed by one or more rubber diaphragms that are pierced by the bullet itself, or are already cross-etched so that they open as it passes through and then close again. This artifice makes it possible to gain some decibels of attenuation since the diaphragms almost completely suppress the precursor wave, but they have the drawback of having to be replaced almost after each shot.
The greatest difficulty in the construction of a silencer consists in the perfect alignment and centering of the internal components with respect to the barrel core so that the bullet passage hole is as small as possible (usually a few tenths of a millimeter larger than the bullet diameter), without compromising the safety of the shooter. In fact, upon exiting the muzzle, the bullet, as mentioned above, may not be well stabilized.
A good silencer does not alter the trajectory of the bullet and does not affect the accuracy of the weapon. If the silencer allows gases to overtake the projectile, turbulence is created that can lead to loss of stability of the projectile; this also occurs in silencers with rubber diaphragms, due to rubbing against them.
A silencer attenuates noise, at most, by 30 dB. The silencer system must be sized to the noise produced (i.e., the more powerful the shot, the bulkier the silencer will have to be or use more sound-absorbing material). A medium-caliber weapon, such as a 9 mm like that carried by the Italian police force, produces a noise of about 140-150 dB. To reduce the noise to reasonable values, indicatively to one-third of the measure expressed in dB (corresponding to an intensity of 100 million to several billion times less), silencers with a diameter between 25 and 40 mm and a length of about 20 to 35 cm must be used, i.e., much longer than a common pistol and obviously bulky compared to the weapon.
Individuals continuously exposed to noise, such as gunfire, are prone to the onset of so-called "noise hearing loss." Therefore, by means of an analytical
experimental study, the authors evaluated any alterations in the hearing of 80 shooters.
## II. MATERIALS AND METHODS
The experimental study conducted focuses on the auditory consequences in patients exposed to the noise of rifle or pistol firing. Forty men working in the gun and using a pistol and 40 men using a rifle for recreational purposes were considered. Specifically, with regard to rifle use, 20 left-handed men and 20 right-handed men were considered. All subjects ranged in age from 20 to 60 years.
The type of gun used, the caliber of the gun, the frequency of firing during the year, subjective and objective hearing examinations, and the change in hearing perception in daily life were then analyzed by administering a questionnaire. All subjects gave accurate answers through face-to-face interview and interactive questionnaire, made through "google forms."
### Interactive Questionnaire
The questions answered remotely by the subjects analyze the lifestyle and daily problems of the subjects suffering from noise hearing loss:
1. Gender
2. Age
3. Recreational or work-type shooting activity
4. Type of weapon used for shooting
5. Frequency of use of noise caps/headsets
6. Limb used to shoot
7. Frequency of firing during the year
8. Worsening of auditory perception since the start of the activity
9. Major difficulties with auditory perception in daily life (e.g., difficulty understanding TV, people, loud music)
10. Report of an audiometric examination performed
11. Any other pathologies associated with the ear
12. Discomfort while listening to noises easily tolerated by other people
The same were then subjected to specialized objective examination, which consists of viewing the ear canal and then performing tonal and speech audiometric examination in a silent booth to assess the audiometric curve.
## III. RESULTS
### a) Subjects using a short Weapon
Regarding the use of a short weapon, the subjects analyzed in this study all work in the armed forces, are male, and use a Beretta model 92 FS brand pistol in 9 PARA (9 x 19 mm) caliber.
All of them reported using ear protectors during firing tests performed at the firing range. In fact, on the specialized objective examination, almost all of the

officers did not show a decrease in hearing due to the protectors used during the firing practice at the range.
In addition, only 8 of them (20%) reported during the interview that they perceived changes related
to their hearing, and thus a change in auditory perception, compared to the period prior to joining the armed forces and then using the weapon.
Table 1: Shows the responses to the questionnaire, as well as the findings of the objective examination performed on the sample of subjects who shoot a gun and are members of the armed corps
<table><tr><td>Patient</td><td>Age</td><td>History of Hearing</td><td>Changes in Hearing Perception</td><td>Headset</td><td>Limb used</td><td>Annual Frequency</td></tr><tr><td>1</td><td>59</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>2</td><td>45</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>3</td><td>49</td><td>mild hearing loss</td><td>recruitment</td><td>sometimes</td><td>right</td><td>2-3 times</td></tr><tr><td>4</td><td>51</td><td>mild hearing loss</td><td>reduced perception of sounds</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>5</td><td>57</td><td>mild hearing loss</td><td>reduced perception of sounds</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>6</td><td>57</td><td>mild hearing loss</td><td>slight hearing loss in everyday life</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>7</td><td>30</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>8</td><td>45</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>9</td><td>43</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>10</td><td>32</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>11</td><td>41</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>12</td><td>42</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>13</td><td>55</td><td>normal-hearing</td><td>slight hearing loss in everyday life</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>14</td><td>31</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>15</td><td>45</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>16</td><td>47</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>17</td><td>50</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>18</td><td>44</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>19</td><td>45</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>20</td><td>42</td><td>mild hearing loss</td><td>slight hearing loss in everyday life</td><td>no</td><td>left</td><td>2-3 times</td></tr><tr><td>21</td><td>51</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>da 4 a 10 times</td></tr><tr><td>22</td><td>39</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>23</td><td>43</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>24</td><td>40</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>25</td><td>42</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>26</td><td>58</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>27</td><td>57</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>28</td><td>33</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>29</td><td>41</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>30</td><td>29</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>31</td><td>35</td><td>normal-hearing</td><td>no</td><td>yes</td><td>left</td><td>2-3 times</td></tr><tr><td>32</td><td>38</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>33</td><td>28</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>34</td><td>50</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>35</td><td>57</td><td>mild hearing loss</td><td>slight hearing loss in everyday life</td><td>yes</td><td>right</td><td>da 4 a 10 times</td></tr><tr><td>36</td><td>43</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>37</td><td>31</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>38</td><td>35</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>2-3 times</td></tr><tr><td>39</td><td>42</td><td>normal-hearing</td><td>no</td><td>yes</td><td>right</td><td>usually</td></tr><tr><td>40</td><td>32</td><td>normal-hearing</td><td>slight hearing loss in everyday life</td><td>yes</td><td>left</td><td>2-3 times</td></tr></table>
Table 2 shows that in only 8 cases (20 percent of the gun-shooting subjects), the same ones who reported impaired auditory perception, there is a noticeable worsening and lowering of the hearing threshold of the ear; in these cases, through a tonal audiometric test, a deep at $4000\mathrm{Hz}$ was observed, given by the gunshots.
Left-handed subjects have slightly more hearing loss in the left ear, but there is no significant difference
from ear to ear. Of paramount importance to consider is the age of the subject. Those examined from about 20 to 40 years of age show no signs of hearing deterioration, especially if they use earplugs. This is likely because with advancing age, degenerative phenomena also intervene, which, together with repeated noise, are responsible for hearing impairment (EVENTUAL BIBLE).
The last column shows the PTA "Pure Tone Average," which is the average of the three thresholds 500 Hz, 1000 Hz. and 2000 Hz. It is a useful value for determining the hearing impairment of the ear.
<table><tr><td>Patient</td><td>Recruitment</td><td>Vocal Curve</td><td>Pta</td></tr><tr><td>1</td><td>no</td><td>normal result</td><td>30 dB</td></tr><tr><td>2</td><td>no</td><td>normal result</td><td>27 dB</td></tr><tr><td>3</td><td>sì</td><td>roll-over</td><td>60 dB</td></tr><tr><td>4</td><td>no</td><td>mild hearing loss</td><td>40 dB</td></tr><tr><td>5</td><td>no</td><td>mild hearing loss</td><td>43 dB</td></tr><tr><td>6</td><td>no</td><td>mild hearing loss</td><td>39 dB</td></tr><tr><td>7</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>8</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>9</td><td>no</td><td>normal result</td><td>28 dB</td></tr><tr><td>10</td><td>no</td><td>normal result</td><td>32 dB</td></tr><tr><td>11</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>12</td><td>no</td><td>normal result</td><td>23 dB</td></tr><tr><td>13</td><td>no</td><td>mild hearing loss</td><td>40 dB</td></tr><tr><td>14</td><td>no</td><td>normal result</td><td>20 dB</td></tr><tr><td>15</td><td>no</td><td>normal result</td><td>27 dB</td></tr><tr><td>16</td><td>no</td><td>normal result</td><td>24 dB</td></tr><tr><td>17</td><td>no</td><td>normal result</td><td>22 dB</td></tr><tr><td>18</td><td>no</td><td>normal result</td><td>29 dB</td></tr><tr><td>19</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>20</td><td>no</td><td>mild hearing loss</td><td>43 dB</td></tr><tr><td>21</td><td>no</td><td>normal result</td><td>30 dB</td></tr><tr><td>22</td><td>no</td><td>normal result</td><td>30 dB</td></tr><tr><td>23</td><td>no</td><td>normal result</td><td>28 dB</td></tr><tr><td>24</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>25</td><td>no</td><td>normal result</td><td>28 dB</td></tr><tr><td>26</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>27</td><td>no</td><td>normal result</td><td>28 dB</td></tr><tr><td>28</td><td>no</td><td>normal result</td><td>20 dB</td></tr><tr><td>29</td><td>no</td><td>normal result</td><td>24 dB</td></tr><tr><td>30</td><td>no</td><td>normal result</td><td>18 dB</td></tr><tr><td>31</td><td>no</td><td>normal result</td><td>21 dB</td></tr><tr><td>32</td><td>no</td><td>normal result</td><td>27 dB</td></tr><tr><td>33</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>34</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>35</td><td>no</td><td>mild hearing loss</td><td>47 dB</td></tr><tr><td>36</td><td>no</td><td>normal result</td><td>20 dB</td></tr><tr><td>37</td><td>no</td><td>normal result</td><td>25 dB</td></tr><tr><td>38</td><td>no</td><td>normal result</td><td>26 dB</td></tr><tr><td>39</td><td>no</td><td>normal result</td><td>30 dB</td></tr><tr><td>40</td><td>no</td><td>mild hearing loss</td><td>39 dB</td></tr></table>
Subjects older than 45 years show hearing impairment, which results in difficulty in perception of soft and high-pitched sounds and reduced understanding of speech. In general, in law enforcement, we do not find particular cases of hearing
loss, except in middle- to older-aged subjects, where we find sensorineural hearing loss, accompanied in speech audiometry by an S-shaped curve shifted more to the right, i.e., toward higher dB, or plateau or roll-over curve, if the auditory nerve is affected.
### b) Subjects using a Long Gun
Men who use a rifle range in age from 30 to 80 years and are all male. Depending on the frequency of their play activity, they have hearing problems. In these cases, unlike the armed forces, the subjects almost never use earplugs, mainly because they need to hear their surroundings to perceive the approach of an animal. Thus, even younger people present hearing problems.
In their medical history they report discomfort in the perception of loud noises, perceived as high but
bearable by normoacoustic people. Some complain of continuous subjective tinnitus and present considerable difficulty in understanding conversations, especially in noisy or crowded environments.
Objective examination shows descending audiometric curves, with medium to severe deafness in older patients, while in younger patients there is a deep at $4000\mathrm{Hz}$. Many of the subjects have recruitment, that is, they have a lowering of the threshold of annoyance, so loud noises are difficult to tolerate.
Patient Age History of Hearing Changes in Hearing Perception Headset Limb Used Marca E Calibro Dell'arma Annual Frequency
<table><tr><td>Patient</td><td>Age</td><td>History of Hearing</td><td>Changes in Hearing Perception</td><td>Headset</td><td>Limb Used</td><td>Marca E Calibro Dell'arma</td><td>Annual Frequency</td></tr><tr><td>1</td><td>43</td><td>bilateral hearing loss</td><td>hearing loss in everyday life</td><td>no</td><td>right</td><td>Franchi 712 VSL caliber 12</td><td>frequently</td></tr><tr><td>2</td><td>75</td><td>bilateral hearing loss</td><td>hea</td><td>no</td><td>right</td><td>Franchi 712 VSL caliber 12</td><td>frequently</td></tr><tr><td>3</td><td>57</td><td>bilateral hearing loss</td><td>hearing loss in everyday life</td><td>no</td><td>right</td><td>Beretta AL390 caliber 12</td><td>2-3 volte</td></tr><tr><td>4</td><td>62</td><td>bilateral hearing loss</td><td>hearing loss in everyday life</td><td>no</td><td>right</td><td>Beretta AL390 caliber 12</td><td>4-10 times</td></tr><tr><td>5</td><td>80</td><td>bilateral hearing loss</td><td>hearing loss in everyday li</td><td>no</td><td>left</td><td>Beretta AL390 caliber 12</td><td>4-10 times</td></tr></table>

<table><tr><td>Patient</td><td>Recruitment</td><td>Vocal Curve</td><td>Pta</td></tr><tr><td>1</td><td>yes</td><td>roll-over</td><td>58 dB</td></tr><tr><td>2</td><td>yes</td><td>roll-over</td><td>65 dB</td></tr><tr><td>3</td><td>no</td><td>normal result</td><td>19 dB</td></tr><tr><td>4</td><td>Yes</td><td>roll-over</td><td>55 dB</td></tr><tr><td>5</td><td>No</td><td>mild hearing loss</td><td>49 dB</td></tr><tr><td>6</td><td>No</td><td>mild heari</td><td>54 dB</td></tr><tr><td>7</td><td>No</td><td>normal result</td><td>25 dB</td></tr><tr><td>8</td><td>No</td><td>normal result</td><td>25 dB</td></tr><tr><td>9</td><td>No</td><td>mild hearing loss</td><td>58 dB</td></tr><tr><td>10</td><td>Yes</td><td>roll-over</td><td>65 dB</td></tr><tr><td>11</td><td>No</td><td>normal result</td><td>21 dB</td></tr><tr><td>12</td><td>No</td><td>mild hearing loss</td><td>49 dB</td></tr><tr><td>13</td><td>No</td><td>mild</td><td>57 dB</td></tr></table>
The graph relates the age of the subjects as a function of the average speech frequency (500- 1000-2000-4000) Hz. It can be seen from the graph that there is a direct proportionality between the two variables in most cases for the presbycus component present.
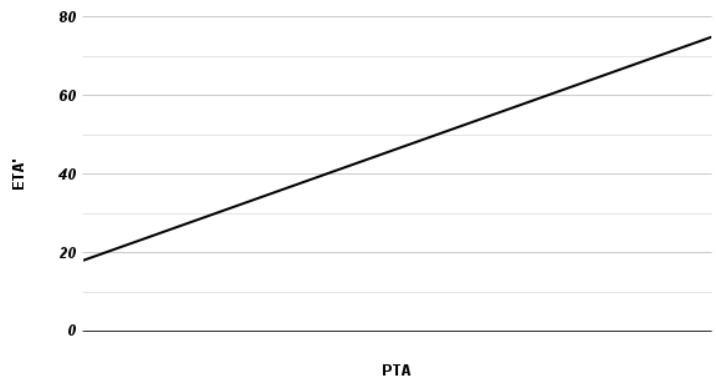
Variazione del calo uditivo rispetto all'ètà
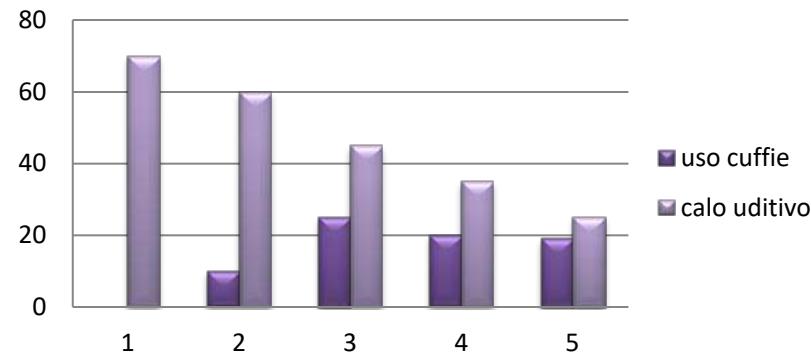
Proporzionalità tra uso cuffie e calo uditivo
The graph above relates hearing loss to the use of protective devices by the subjects examined. It can be easily deduced that noise-exposed subjects with protection by means of ear muffs (or earplugs) had significantly less hearing loss than those who did not use them. In this study, it was also found that it is the hunters who clearly use the protective devices less, as they need to hear the surrounding noise, while the subjects who work/have worked in the weapon, rarely shoot without earphones/plugs, being on average $80\%$ of their activity performed in the ranges.
It is noted, in subjects exposed to gunfire noise, regardless of caliber, without ear protectors, a hearing deficit, with, in the early stages, a deep visible by tonal audiometry, on the frequency of $4000\mathrm{Hz}$. Thereafter, the curve begins to take the "downward" shape, and the subject begins to have difficulty perceiving soft and high-pitched sounds. In the last stage he will also lose the low sounds (125Hz, 250Hz, 500Hz), taking into account the subject's age, which will be more advanced. So, of fundamental importance is the age of the subject, which is the cause of presbycusis, thus the aging and death of hair cells through physiological aging, an aspect that should not be underestimated since it easily affects the psychological and social sphere of the subject, causing isolation and, in more severe cases, senile dementia.
In addition, the more frequent the exposure to noise, the greater the hearing damage, the faster the decay and death of hair cells. By voice audiometry, a curve shifted toward higher dB intensities is noted in the early stages of hearing loss (mild hearing loss), the curve rolls-over as the person becomes increasingly exposed to gunshots (in the absence of protection) and the deficit worsens, the curve turns to roll-over when the nerve is now involved. The person perceives subjective tinnitus and, in more severe cases, the phenomenon of recruitment appears, recognized by specific hearing tests mentioned above. Individuals who use hearing protectors, on the other hand, are less likely to be
affected by noise-induced hearing loss, especially if the time of noise exposure is minimal.
## IV. DISCUSSION
Individuals who are continuously exposed to noise, such as gunfire, are prone to the onset of so-called "gun-shooting hearing loss." [9]. Noise-induced hearing loss is the most common occupational disease in Italy, characterized by irreversible cochlear impairment resulting from prolonged exposure to high sound levels. [10]. Specifically, there is a loss of outer hair cells and subsequent neuronal degeneration. This definition excludes deafness from acute sound trauma, which falls under the umbrella of occupational accidents, but also accidental hearing injuries from explosion or barotrauma, whose etiopathogenic mechanism is different.
Noise-induced hearing loss is a bilateral, as a rule symmetrical, sensorineural hearing loss arising from broadband and/or intermittent-acting impulsive noise of $>80 - 85$ dB with a daily exposure duration of 6-8 hours for several years. [11]. Magnitude and progression of hearing damage depend on overload parameters (noise intensity, duration of its action, frequency components) as well as on the duration of interval phases (noise breaks) and individual sensitivity. So, we find a perceptual type of hearing loss, bilateral and symmetrical, with deep (falling) on $3000 / 4000\mathrm{Hz}$ and rising on $8000\mathrm{Hz}$ in the early phase (according to recent studies at least $40\%$ of hearing losses from chronic acoustic trauma show a downward curve). The developmental course of hearing damage from noise is also characteristic: the elevation of the hearing threshold, i.e., the worsening of hearing loss detectable by tonal audiometry, may be relevant especially in the first 10 years of continued noise exposure and then stabilize; the tonal audiometric tracing faithfully follows the progression of damage to the neuroepithelium of the basal gyrus of the cochlea. What is thus evident is a
bilateral perceptual hearing loss with substantial "tightness" of low and mid frequencies and threshold elevation from 2000 Hz to 8000 Hz in the more advanced forms. [12].
### a) Prosthesisization
Prosthetic therapy finds indication in all cases of hearing loss. In fact, prosthesisization is commonly indicated in cases where the deficit is of such a magnitude that it results in discomfort for the patient and where there is no room for a pharmacological solution [13]
The choice of hearing aid is up to the hearing aid technician, on whom the future wearer of the device relies. This choice depends, first and foremost, on the severity of the hearing impairment and the lifestyle of the wearer. People with severe hearing impairment need powerful hearing aids. Hence, behind-the-ear aids are indicated. Conversely, if the deficit is mild (especially in pantalal deafness) an in-the-ear hearing aid may be opted for. [14].
With mild to moderate hearing impairment, consideration of the patient's lifestyle is important. For active people (e.g., young people), an in-the-ear hearing aid is the best choice, as the latter allows more freedom of movement. Conversely, for people who are sedentary or less adept at handling electronic devices (e.g., elderly), the best choice is generally the behind-the-ear type hearing aid, as it is easy to remove and manage. Usually, in people with noise-induced hearing impairment, behind-the-ear hearing aids are recommended, as the latter, compared with in-the-ear, give less sensation of "closing" and try to mask the patient's tinnitus by means of a sound stimulus originating from the device. [15, 16].
Prosthesisization must obviously be preceded by a functional study that is based on:
- Tonal audiometry: to define the extent of the hearing deficit, the trend of the audiometric curve, the type of deficit [17];
- Supraliminary audiometry: in order to show whether, in case of sensorineural deficit, there is pathological recruitment or adaptation [18].
- Search for the threshold of stapedius reflex evocation: a threshold that is about 10 Db below the threshold of annoyance that should not be exceeded by amplification [19, 20]
- Speech audiometry: in order to define discriminative potential by increasing the acoustic intensity level.
The presence of recruitment can be compensated for by the introduction of prosthesis gain limitations.
Prosthesizing a noise hearing loss is one of the most challenging tasks for rehabilitative audiology. Hearing loss is limited to high frequencies with constant
presence of recruitment and often tinnitus, this causes altered sound perception. [21, 22].
### b) Assessment in the Medico-Legal Context
The medico-legal assessment of hearing loss in civil liability [23] distinguishes the assessment of complete deafness, unilateral or bilateral, from that of deaf-mutism, due to inability, in the latter case, to acquire adequate language in the developmental stage. The damage rate corresponds to $10\%$ for unilateral complete deafness and $50\%$ for bilateral complete. The evaluation of intermediate hearing deficits, which must necessarily consider that in the range between 45 and 65 dB the impairment of social auditory function is rapidly progressive, assigns a percentage of damage in relation to the frequencies and dB considered according to the following table:
The assessment of hearing ability must be carried out on a prosthetically implanted individual and involves the assignment of a damage plus of $2 - 6\%$ in relation to disesthetics and limitations in daily activities resulting from the prosthesis.
In the case of unilateral intermediate hearing deficit, the overall assessment of the reduction in psychophysical integrity should be calculated according to the proportion: "deficit: 100 = psychophysical integrity: 10," where D is the percentage of hearing deficit and I is the reduction in psychophysical integrity.
The assessment of bilateral intermediate hearing deficit involves the overall calculation of impairment according to the formula: $[(4 \times \text{best ear deficit}) + \text{worst ear deficit}] / 5 \times 0.50$.
Regarding the assessment of hearing impairment in the care setting, the reference standard is Italian Ministry of Health Ministerial Decree No. 463800, 05.02.1992. The aforementioned decree specifies that the deafness entitling to the recognition of welfare benefits is that acquired in developmental age that prevents normal learning of spoken language, commonly referred to as prelingual deafness. Regarding the time limits of developmental age, the Ministerial Decree identifies the time span from birth to the age of 12. The medico-legal evaluation is to be carried out by performing oto-functional examinations with the naked ear, i.e., without a prosthesis. The score for hearing impairments with a fluctuating and discontinuous pattern over time must result from a 12-month observation period with average hearing loss assessed on 3 oto-functional examinations performed every 3-4 months.
In assigning the overall percentage of civil disability, the Italian Ministerial Decree 05.02.1992 assigns a score of $15\%$ to unilateral total deafness and $58.5\%$ if bilateral total. Unilateral/bilateral hearing losses equal to or less than 245 dB will have to be evaluated by calculating the sum of hearing losses in dB for the frequencies 500, 1000 and $2000\mathrm{Hz}$. The overall
percentage of disability will be given by the value calculated by crossing the data of the worst ear (ordinate) with the best ear (abscissa).
For the purpose of granting the nonreversible pension [24] recognition of congenital or acquired deafness during developmental age with hearing loss equal to or greater than 75 dB HTL of average between the frequencies 500, 1000 and $2000\mathrm{Hz}$ in the better ear. Upon reaching the age of 65, the pension turns into a replacement social allowance.
Additional welfare benefit for the deaf is the communication allowance, provided for by Italian Law 508/1988, which can be granted to the applicant under the age of 12 with a hearing loss equal to or greater than 60 dB of HTL averaged between the frequencies 500, 1000 and $2000\mathrm{Hz}$ in the better ear. If the applicant is above this age, the hearing loss must be 75 decibels HTL or more and the onset of hearing loss must be demonstrated before the age of 12.
In the context of occupational accidents and diseases, the medico-legal assessment of hearing loss uses as benchmarks the values indicated in the table attached to Italian Legislative Decree No. 38/2000 (commonly known as the "INAIL 2000" tables). In that normative source, the percentage value assigned to unilateral complete hearing loss is $12\%$, while bilateral complete deafness is assigned a value of $50\%$. With regard to the assessment of biological damage of bilateral partial hearing impairment, the formula "Biological damage = (best ear x 4) + worst ear x 0.5" is applied, using the values inferable from the attached table (it should be noted that the values given are super impossible on those provided by the SIMLA guidelines on the assessment of personal injury in civil law):
This evaluative procedure operates an assessment of unilateral hearing impairment on the basis of the assumption that auditory impairment is in fact impairment of sensory organ function, where in the descriptive definition of sensory organ comes to include, in the case of the ear, also the more extensive conceptual definition of equal organ as an entity, on the functional level, distinct from the pure anatomical entity for the correspondence "of function" that it performs with another organ that, morphologically, is repeated in the other half of the body. For the purposes of auditory function, organ parity (better ear vs. worse ear) results, therefore, in the expression of an "organ-functional system," i.e., an anatomical-functional system in which all anatomical structures are called upon to perform similar sensory functions [25]. In Inail, for assessment purposes, permanent impairment of the hearing organ is assessed when the average of hearing losses on the frequencies 5000-1000-2000-3000-4000 Hz is greater than 25 dB.
### c) The Goals of Prosthetics
The first goal to be achieved in the prosthetic strategy in general and in noise-induced hearing loss in particular is to improve the signal-to-noise ratio (SNR).
First-generation hearing aids all have excellent and powerful amplification, controls for controlling "peak clipping" and compression of the sound signal, but non-frequency-selective linear amplification, by also raising background noise, causes distortion of the sound message with alteration of verbal intelligibility and thus comprehension [26]. Hearing aids that are digitally "programmable" by computer, although the processing of the sound signal continues to be analog, have some additional functions that allow some of the potential of the hearing aid to be improved, for example, using a program for directional listening (if you are talking to someone) or a program that allows omnidirectional listening (if you want to listen to music). This is possible and feasible if the signal is pure, i.e., does not contain added noise but only words or music. In everyday life this situation is uncommon. With the advent of digital technology it is possible to separate the voice from the noise, that is, unpacking the signifying signal from any noise elements. One no longer has a single amplification channel but a division into bands of the frequency spectrum, each with its own amplitude and compression characteristics. In a digital multiband system, it is possible to analyze the amplitude envelope of the entire frequency spectrum, identify the channels where noise is predominant, then work out a special algorithm that reduces the gain only at these bands, leaving unchanged-or increasing-the sound level for the band where the voice predominates." It is then possible to create amplification on different channels and with different characteristics (compression ratio, threshold, attack and recovery times) depending on the patient's dynamic residual hearing range. In cases of noise deafness, the most beneficial device is the behind-the-ear device: BTE (receiver behind the ear), RITE (with receiver inside the ear) or MINI RITE; progressively smaller in size. Depending on the quality of the device, one can adjust multiple frequency channels, program the device for tinnitus, and improve the sensation given by recruitment [27].
However, if the hearing loss is mild and the subject is not subject to any particular auditory consequences given by the noise, a fitting with in-the-ear devices can be done. Important is the willingness of the subject, the only one who can balance quality, design and effectiveness of the device.
## V. CONCLUSION
In individuals with noise-induced hearing loss, prosthesizing by means of behind-the-ear hearing aids is very effective. Hearing aids, in milder cases, make people rediscover sounds that have become inaudible;
in more severe cases, they attempt to reduce the recruitment and perception of tinnitus, through specific programs. Firststep, of fundamental importance remains that of prevention to hearing loss, in work environments using the appropriate protective equipment (noise-cancelling headphones, ear protectors) and in recreational environments, if it is not possible to use protective devices, limit noise exposure.
From the medico-legal point of view, depending on the area in which one is, it is necessary to assess the extent of the damage that has been established in order to grant him fair economic compensation. A critically important factor to be considered for compensation is whether prosthetics have been used.
Generating HTML Viewer...
References
27 Cites in Article
W Snow (1967). Survey of acoustic characteristics of bullet shock waves.
Z Bro Ek-Mucha,K Zdeb (2017). Controversial Suicide Case Using a Submachine Gun with a Sound Suppressor-The Need for Team Work of Forensic Chemistry and Firearm Examiners.
Richard Raspet (1998). Shock Waves, Blast Waves, and Sonic Booms.
Roland Stoughton (1997). Measurements of small-caliber ballistic shock waves in air.
K Lo,B Ferguson (2012). Localization of small arms fire using acoustic measurements of muzzle blast and/or ballistic shock wave arrivals.
D Samsonov,J Goree,H Thomas,G Morfill (2000). Mach cone shocks in a two-dimensional Yukawa solid using a complex plasma.
Robert Maher (2007). Acoustical Characterization of Gunshots.
J Freytag,B Brustad (2005). A survey of audio forensic gunshot investigations.
J Sataloff,M Hawkshaw,R Sataloff (2010). Gunshooting hearing loss": A pilot study.
Małgorzata Pawlaczyk-Łuszczyńska,Adam Dudarewicz,Kamil Zaborowski,Małgorzata Zamojska-Daniszewska (2004). Noise exposure and hearing status among employees using communication headsets.
(2014). Hearing Loss and Older Adults.
John Lasak,Patrick Allen,Tim Mcvay,Douglas Lewis (2013). Hearing Loss.
M Ylikoski,J Pekkarinen,J Starck,R Pääkkönen,J Ylikoski (1995). Physical characteristics of gunfire impulse noise and its attenuation by hearing protectors.
U Hoppe,G Hesse (2017). Hearing aids: indications, technology, adaptation, and quality control.
Lars Haab,Caroline Lehser,Farah Corona-Strauss,Corinna Bernarding,Harald Seidler,Ronny Hannemann,Daniel Strauss (2019). Implementation and Long-Term Evaluation of a Hearing Aid Supported Tinnitus Treatment Using Notched Environmental Sounds.
Del Bo,L Ambrosetti,U (2007). Hearing aids for the treatment of tinnitus.
E Pirodda (1951). Audiometria Tonale [Tonal audiometry.
Z Hribar,Pompe (1956). Nasa opazanja kod nekih supraliminarnih audiometrijskih testova [Personal observations on supraliminary audiometric tests.
T Matsui (1980). Stapedius reflex].
László Tóth,Tamás Rácz,Péter Diószeghy,Gábor Répássy,István Lampé (2000). Otoacoustic emission in myasthenia gravis patients and the role of efferent activation.
R Ivory,R Kane,R Diaz (2014). Noise-induced hearing loss: a recreational noise perspective.
Emily Stucken,Robert Hong (2014). Noise-induced hearing loss.
(2014). Guidelines for the medico-legal assessment of personal injury in civil law -SIMLA.
Shinhong Min (1970). The Relationship between Parenting stress, Parenting efficacy, and Resilience in Mothers with Early school-age children.
Carlo Bracci,Gabriele Norcia (2014). Evaluation of Work-related Diseases by the Italian Institute of Insurance for Professional Illness and Injuries(INAIL).
T Crain,Van Tasell,D (1994). Effect of peak clipping on speech recognition threshold.
J Ng,A Loke (2015). Determinants of hearing-aid adoption and use among the elderly: a systematic review.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Benedetta Pia De Luca. 2026. \u201cDamage of Auditory Perception Following Firearm Use: An Experimental Study Conducted on 80 Patients\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 24 (GJMR Volume 24 Issue K3): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.