## I. INTRODUCTION
Down Syndrome (DS), also known as Trisomy of Chromosome 21, is a condition characterized by the presence of an extra chromosome 21, resulting in trisomy $21^{1-6}$. There are three ways in which this genetic anomaly can occur: free trisomy (error in division during meiosis), Robertsonian translocation (fusion of chromosomes 13, 14, 15 with 21), and mosaicism (presence of both normal and trisomic cells at the same time). It is the most common genetic anomaly worldwide, with an incidence of 10-14 per 10,000 live births<sup>4-8</sup>.
The physical characteristics of individuals with DS include short stature, shortened extremities (hands, feet, fingers, nose, and ears), a single transverse palmar crease, wide spacing between the first and second toes with a deep groove near the plantar surface, underdeveloped genitals, brachycephaly, a wide and short neck, almond-shaped eyes that are relatively distant from each other, oblique palpebral fissure, inability to seal the lips completely, narrow nasal bridge and nasopharynx, low-set ears, prominent cheeks, adenotonsillar hypertrophy, and thin and sparse hair. They generally have a docile and affectionate temperament $^{9-12}$.
Individuals with DS may also experience generalized muscular hypotonia, congenital heart disease, pulmonary hypertension, obstructive sleep apnea, hearing and vision impairments, thyroid disorders (75% hypothyroidism and 6% hyperthyroidism), diabetes, obesity, motor deficits, celiac disease, neurological issues with language and cognitive delays, epilepsy in 26% of cases, and premature aging that can lead to Alzheimer's disease. Gastrointestinal disorders, such as necrotizing enterocolitis, may also be present in 16% of newborns. Hypovitaminosis D and low bone mineral density can lead to osteoporosis in adults. The altered immune system in individuals with DS makes them more susceptible to infections $^{1,3-5,7-8,10,13-18}$.
In terms of oral changes, individuals with DS may exhibit mouth breathing, xerostomia, narrow maxilla, mandibular protrusion, narrow and deep palate, fissured lips and tongue, macroglossia, temporomandibular dysfunction, and malocclusion, with Class III and unilateral or bilateral crossbites being the most common. Dental structure abnormalities such as agenesis, delayed tooth eruption, taurodontia, microdontia, hypodontia, hyperdontia, and enamel hypoplasia are also observed. There is a higher prevalence of premature periodontal disease, tooth exfoliation, gum bleeding, candidiasis, cheilitis, and acute necrotizing ulcerative gingivitis. These characteristics can impact chewing, speech articulation, swallowing, and speech abilities $^{3,10,19}$. Recent studies suggest that individuals with DS have differences in their oral microbiota, with lower levels of Streptococcus mutans in their saliva $^{3}$.
Dental surgeons play a crucial role in maintaining the oral health of these patients, requiring the use of specialized techniques and attention during consultations, particularly regarding the type of medication used $^{19}$. Specific diseases such as diabetes, celiac disease, and leukemia can also have oral implications that demand dental attention $^{10}$. Another example is the use of expanders in the first year of life to stimulate jaw development, muscular and lingual strength, and improve airway clearance, sleep quality, and tongue positioning $^{2,12,19}$. Therefore, it is essential for dental professionals to have knowledge about DS, its systemic implications, and oral characteristics, as well as specific skills needed to provide appropriate care for these patients. This research aimed to investigate the physical, systemic, and stomatological characteristics of individuals with Down Syndrome.
## II. METHODS
### a) Study Design and Ethical Considerations
A descriptive, observational, and cross-sectional study was conducted on a convenience sample of individuals diagnosed with Down Syndrome. Volunteers underwent structured interviews with their responsible caregivers. This study was approved by the Institutional Research Advisory Committee (CAPI) and Research Ethics Committee (CEP) of UNOESTE, under protocol number 023415. Informed consent was obtained from the guardians before the evaluation of the individuals.
### b) Study Population
A total of 42 individuals with Down Syndrome, aged between 0 and 18 years, participated in the study.
Data collection occurred at the Dental Specialties Center of Presidente Prudente. Inclusion criteria included individuals aged 0-18 years, diagnosed with Down Syndrome, and written consent from responsible caregivers to participate in the research.
### c) Clinical Examination
Responsible guardians were interviewed to assess oral hygiene practices and behavioral characteristics of the volunteers. Additionally, systemic conditions, general physical health, dental status, and stomatological features were evaluated.
### d) Stomatological Evaluation
The amount of visible biofilm on the teeth surfaces of the volunteers was assessed using an index $^{20}$, which assigned scores from 0 to 5 based on biofilm thickness and adhesion. Gingival health status was evaluated using a sterile periodontal probe, with scores ranging from 0 to 2 based on the presence and severity of gingivitis. The International Caries Detection and Assessment System was utilized to classify tooth surface conditions and identify carious lesions $^{21}$. The Invasive Needs Index (INI) $^{22}$ was employed to determine the extent of involvement of teeth with active carious lesions requiring invasive treatment.
### e) Statistical Analysis
Descriptive analyses of the data included absolute and relative frequencies, with quartiles calculated for the ICDAS and INI indices. All statistical analyses were performed using the R program $^{23}$. The significance level chosen was $5\%$ $(p = 0.05)$.
## III. RESULTS
In Table 1, it was observed that $52.4\%$ of the sample is male, with the majority being white $(83.3\%)$ and illiterate $(66.7\%)$. The average age of the sample is 12.4 years, a minimum of 5 and a maximum of 18 years.
Table 1: Descriptive Analysis of Participants' Demographic and Literacy Characteristics (n=42)
<table><tr><td>Variable</td><td>Category</td><td>Frequency (%)</td></tr><tr><td rowspan="2">Gender</td><td>Masculine</td><td>22 (52.4%)</td></tr><tr><td>Feminine</td><td>20 (47.6%)</td></tr><tr><td rowspan="4">Race</td><td>White</td><td>35 (83.3%)</td></tr><tr><td>Brown</td><td>2 (4.8%)</td></tr><tr><td>Black</td><td>4 (9.5%)</td></tr><tr><td>Yellow</td><td>1 (2.4%)</td></tr><tr><td rowspan="2">Literate</td><td>No</td><td>28 (66.7%)</td></tr><tr><td>Yes</td><td>14 (33.3%)</td></tr><tr><td></td><td>Mean (standard</td><td>Median (minimum value –</td></tr><tr><td>Age years)</td><td>12.4 (7.9)</td><td>9.5 (5.0 – 18.0)</td></tr></table>
Regarding systemic conditions (Table 2), it is observed that the majority have respiratory diseases $(71.4\%)$, overweight or obesity $(59.5\%)$, heart disease $(57.1\%)$ and obstructive sleep apnea $(54.8\%)$. It is hygiene and $61.9\%$ have a behavioral barrier making hygiene and $61.9\%$ have a behavioral barrier making dental care difficult.
Table 2: Frequencies and Percentages of Sample Participants According to Systemic Conditions (N=42)
<table><tr><td>Variable</td><td>Frequency (%)</td></tr><tr><td>Respiratory diseases</td><td>30 (71.4%)</td></tr><tr><td>Overweight or obesity</td><td>25 (59.5%)</td></tr><tr><td>Heart disease</td><td>24 (57.1%)</td></tr><tr><td>Obstructive sleep apnea</td><td>23 (54.8%)</td></tr><tr><td>Hypothyroidism</td><td>17 (40.5%)</td></tr><tr><td>Atlanto-occipital instability</td><td>13 (31.0%)</td></tr><tr><td>Gastrointestinal disorders</td><td>9 (21.4%)</td></tr><tr><td>Anemia</td><td>7 (16.7%)</td></tr><tr><td>Convulsion</td><td>5 (11.9%)</td></tr><tr><td>Diabetes</td><td>3 (7.1%)</td></tr><tr><td>Hyperthyroidism</td><td>0 (0.0%)</td></tr><tr><td>Does not allow assistance due to behavioral barriers</td><td>26 (61.9%)</td></tr><tr><td>Difficulty brushing</td><td>17 (40.5%)</td></tr></table>
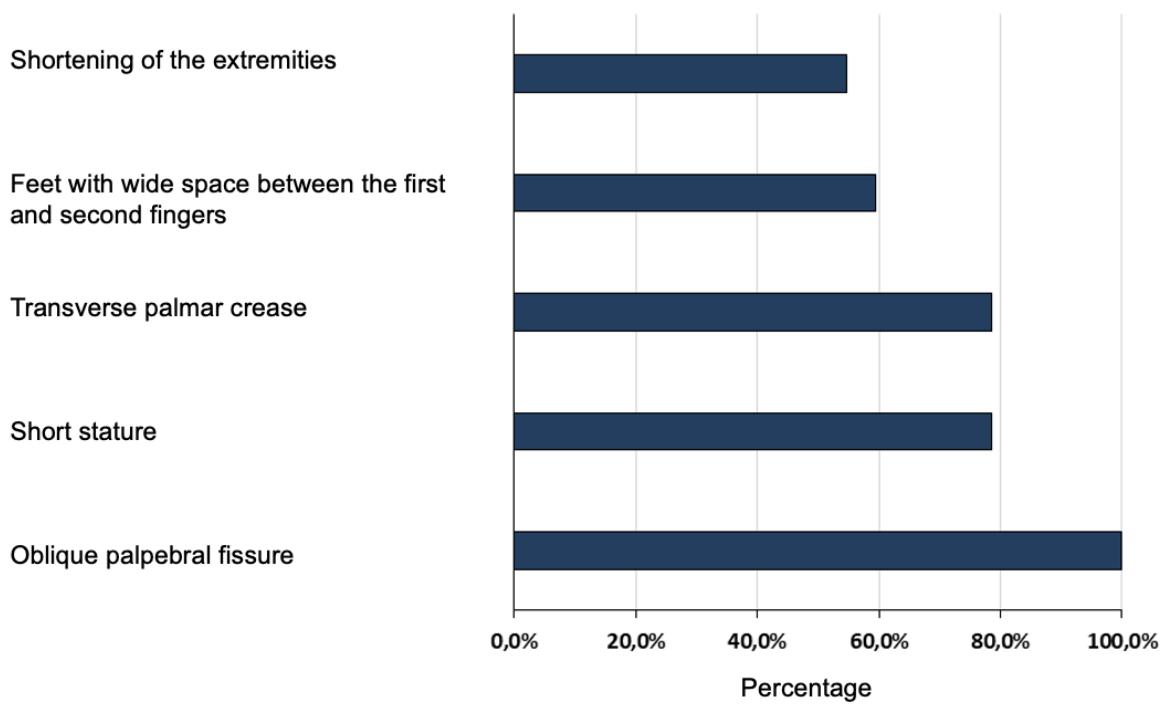
In Figure 1 it can be seen that all participants have an oblique palpebral fissure (100.0%) and the majority have short stature (78.6%), a single transverse palmar crease (78.6%), feet with wide space between the first and second fingers (59.5%) and shortening of the extremities (hands, feet, fingers, nose and ears) (54.8%).
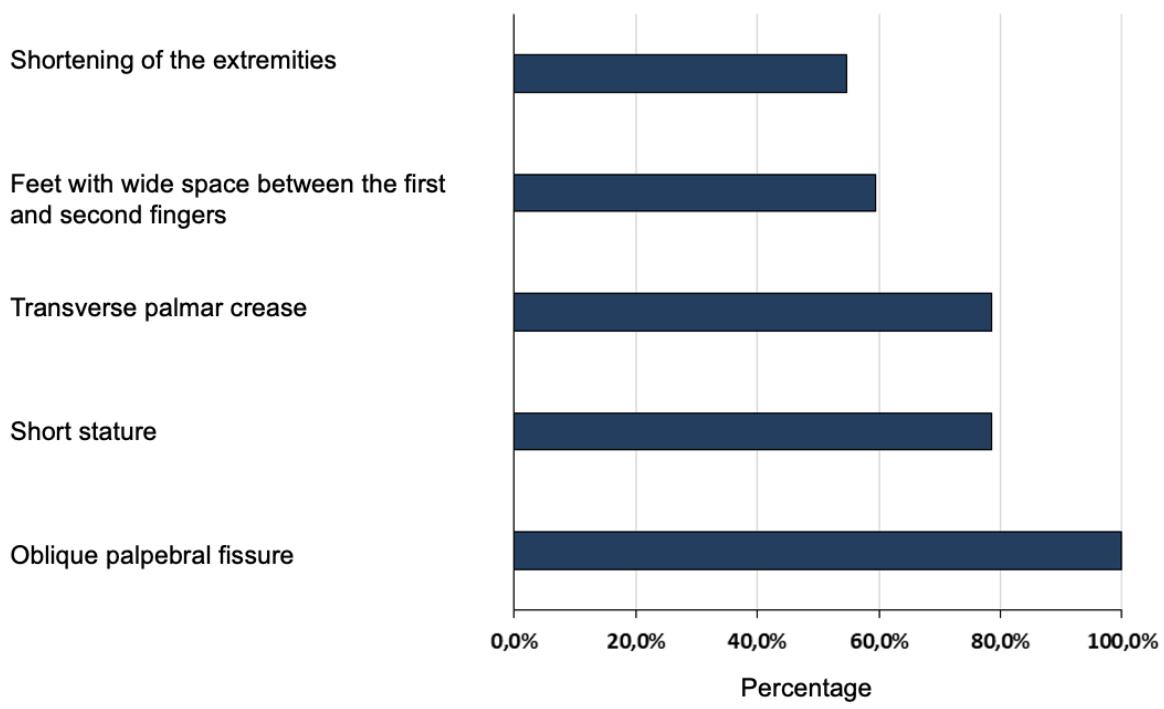 Figure 1: Percentage of Participants In Relation to Physical Characteristics (N=42)
Regarding oral characteristics (Table 3), it is noted that the majority have macroglossia $(69.0\%)$, bruxism $(61.9\%)$ and microdontia $(57.1\%)$. Furthermore, half of the sample had a conoid tooth $(50.0\%)$ and prolonged retention (50.0%). It is also noted that $45.2\%$ have agenesis and $45.2\%$ have a fissured tongue.
Table 3: Frequencies and Percentages of Sample Participants According to Oral Characteristics (N=42)
<table><tr><td>Variable</td><td>Frequency (%)</td></tr><tr><td>Macroglossia</td><td>29 (69.0%)</td></tr><tr><td>Bruxism</td><td>26 (61.9%)</td></tr><tr><td>Microdontics</td><td>24 (57.1%)</td></tr><tr><td>conoid tooth</td><td>21 (50.0%)</td></tr><tr><td>Extended retention</td><td>21 (50.0%)</td></tr><tr><td>Agenesis</td><td>19 (45.2%)</td></tr><tr><td>fissured tongue</td><td>19 (45.2%)</td></tr><tr><td>Angular cheilitis</td><td>10 (23.8%)</td></tr><tr><td>Fusion</td><td>2 (4.8%)</td></tr><tr><td>Supernumerary</td><td>1 (2.4%)</td></tr><tr><td>Macrodontics</td><td>0 (0.0%)</td></tr><tr><td>Twinning</td><td>0 (0.0%)</td></tr></table>
Table 4 presents the results of biofilm indexes, gingival condition, caries experience (ICDAS) and need for treatment. It can be seen that $45.2\%$ of the sample had the biofilm index classified as deficient. Furthermore, $42.9\%$ and $9.5\%$ have mild and severe gingivitis, respectively. Regarding ICDAS, it is observed that $47.6\%$ have index 0, no or little change in enamel translucency. It is also observed that $47.6\%$ present some need for treatment, with $11.9\%$ requiring extraction due to an extensive carious lesion while $52.4\%$ do not need any treatment.
Table 4: Distribution of Sample Participants According to Biofilm Indexes, Gingival Condition, Caries Experience and Need for Treatment (N=42)
<table><tr><td>Variable</td><td>Frequency (%)</td></tr><tr><td>Macroglossia</td><td>29 (69.0%)</td></tr><tr><td>Bruxism</td><td>26 (61.9%)</td></tr><tr><td>Microdontics</td><td>24 (57.1%)</td></tr><tr><td>conoid tooth</td><td>21 (50.0%)</td></tr><tr><td>Extended retention</td><td>21 (50.0%)</td></tr><tr><td>Agenesis</td><td>19 (45.2%)</td></tr><tr><td>fissured tongue</td><td>19 (45.2%)</td></tr><tr><td>Angular cheilitis</td><td>10 (23.8%)</td></tr><tr><td>Fusion</td><td>2 (4.8%)</td></tr><tr><td>Supernumerary</td><td>1 (2.4%)</td></tr><tr><td>Macrodontics</td><td>0 (0.0%)</td></tr><tr><td>Twinning</td><td>0 (0.0%)</td></tr></table>
$^{1}$ ICDAS: International Caries Detection and Assessment System (0: No or little change in enamel translucency; 1: visible initial change in enamel; 2: clear change visible in wet enamel or beyond areas of pits and fissures; 3: discontinuity (microcavity) located in the enamel that may appear opaque or discolored. 4: Shadowing of the underlying dentin; 5: Clear cavity with visible dentin; 6: Clear extensive cavity with visible dentin (involving more than half of the surface). $2^{<\text{NI}}$: Invasive Needs Index (0: No need for treatment; 1: Atraumatic Restorative Treatment (ART); 2: Conservative Pulp Therapy (TPC), PPD, Pulpotomy; 3: Radical Endodontic Treatment; 4: Exodontia for Extensive Carious Lesions (Exo).
## IV. DISCUSSION
Given the results observed, table 1 shows a higher frequency of illiterate patients. Studies indicate that these individuals have the capacity to learn and acquire new skills, but at a slower rate. From the first years of life until early adulthood they have good cognitive development, but as they age, they may experience a decrease in their abilities associated with a possible process of dementia $^{9}$. Approximately $65\%$ of patients with the syndrome may be affected by cognitive impairment that can be observed through understanding and producing language. As a consequence, this can affect communication and understanding between a patient with Down syndrome and the dentist in a dental clinic[24].
In relation to systemic characteristics (Table 2), the results showed a difference in the frequency of respiratory diseases, reaching $71.4\%$, while in another study it was demonstrated a rate of up to $36\%$. Research estimates that overweight or obesity in these individuals may be associated with a slow basal metabolism, hypothyroidism or inadequate eating habits $^{18}$. In the results above, $59.5\%$ of overweight or obesity and $40.5\%$ of hypothyroidism were observed, which may indicate a relationship between these factors.
In patients with DS, the congenital heart defect is widely observed in $40\%$ to $60\%$ of individuals, which is confirmed in this research with $57.1\%$ (Table 2), highlighting the importance of an early diagnosis of this condition to reduce the rates of morbidity and mortality[16]. Furthermore, cardiac patients are at greater risk of developing Infectious Endocarditis when undergoing invasive procedures, due to transient bacteremia and the deposition of microorganisms in compromised cardiac tissues, and the use of antibiotic prophylaxis is recommended according to the American Heart Association protocol. When these patients undergo cardiovascular surgery, they may use oral anticoagulants, increasing the chance of bleeding during dental surgical procedures[125].
Bacterial endocarditis is a severe and life-threatening human infection. Patients at risk for this infection include those with congenital heart disease (CHD), such as individuals with Down syndrome, with the primary etiological factors being microorganisms found in the oral cavity[26].
Another characteristic that has a high prevalence in the literature and proven in the results above is obstructive sleep apnea (Table 2) with around $30\%$ to $60\%$ often associated with macroglossia (11), the use of maxillary expanders has been used for effective treatment[19]. It was also observed that $61.9\%$ of patients with DS presented behavioral barriers with difficulty in receiving care (Table 2), this is due to high rates of hyperactivity, agitation, tantrums and impulsivity. According to the literature, these individuals have better visual than verbal learning, the association of objects as rewards and positive reinforcement are ways to increase their responsiveness[9].
The physical characteristics found were oblique palpebral fissure, short stature, single transverse palmar crease, feet with wide space between the first and second toes and shortening of the extremities (Figure 1), which reinforces the present literature $^{1,5}$. The following oral characteristics were found most frequently: macroglossia, bruxism, microdontia, conoid teeth, prolonged retention, agenesis and fissured tongue (Table 3), which reinforces characteristics described in other studies $^{3,19,27}$. Bruxism $^{27}$, prolonged retention and agenesis are associated with occlusal changes that can occur in these patients $^{12}$.
In table 4, the presence of biofilm (45.2%), mild gingivitis (42.9%) and severe gingivitis (9.5%) was observed in patients with DS, proving the relationship between these two factors and also demonstrating their association with difficulty in cleaning.
The low prevalence of caries is a factor reported in studies that can be proven by the results obtained in this research with the presence of $47.6\%$ in the ICDAS zero index, this would be justified by prolonged retention, agenesis, change in the chronology of tooth eruption, differences in salivary flow, microbiota, pH, buffering capacity/saliva composition and presence of microdontia. However, $42.9\%$ had ICDAS above 3, that is, with shadowing of the subadjacent dentin, a clear cavity in visible dentin or a clear extensive cavity with visible dentin, which is also reported in a smaller number of studies. This condition may be related to factors such as: poor hygiene, less manual dexterity, less access to dental care, use of medication, inadequate diet and negligence on the part of caregivers.
## V. CONCLUSION
Patients with Down Syndrome are characterized by specific physical, systemic, and stomatological traits that may impact oral health, hygiene maintenance, and behavior during dental treatment. The findings indicate prevalent and significant dental necessities in individuals with DS. Notably, a high proportion of subjects exhibited poor oral hygiene (45.2%) and mild gingivitis (42.9%). Furthermore, a majority of participants displayed distinctive oral features, including macroglossia (69.0%), bruxism (61.9%), and microdontia (57.1%). Common systemic conditions among these individuals encompass respiratory ailments (71.4%), overweight or obesity (59.5%), and cardiac anomalies (57.1%). These outcomes underscore the importance of a tailored and specialized dental approach to address the unique requirements of this patient population.
### Declaration of Interest
The authors report no conflict of interest.
Generating HTML Viewer...
References
28 Cites in Article
A Blanco-Montaño,M Ramos-Arenas,B Yerena-Echevarría,Miranda-Santizo Ld,Ríos-Celis,A,Dorantes-Gómez At,A Morato-Rangel,J Meza-Hernández,E Acosta-Saldívar,C Aguilar-Castillo,A Cárdenas-Conejo (2023). Factores de riesgo en el origen del síndrome de Down [Risk factors in the origin of Down syndrome.
Peter Schmidt,Laura Suchy,Andreas Schulte (2022). Oral Health Care of People with Down Syndrome in Germany.
Amy Tsou,Peter Bulova,George Capone,Brian Chicoine,Bryn Gelaro,Terry Harville,Barry Martin,Dennis Mcguire,Kent Mckelvey,Moya Peterson,Carl Tyler,Michael Wells,Michelle Whitten (2020). Medical Care of Adults With Down Syndrome.
K Dimopoulos,A Constantine,P Clift,R Condliffe,S Moledina,K Jansen,R Inuzuka,G Veldtman,C Cua,Elw Tay,A Opotowsky,G Giannakoulas,R Alonso-Gonzalez,R Cordina,G Capone,J Namuyonga,C Scott,D 'alto,M Gamero,F Chicoine,B Gu,H Limsuwan,A Majekodunmi,T Budts,W Coghlan,G Broberg,C (2023). for Down Syndrome International (DSi). Cardiovascular Complications of Down Syndrome: Scoping Review and Expert Consensus.
M Bull,T Trotter,S Santoro,C Christensen,Rw; Council On Genetics; Grout,L Burke,S Berry,T Geleske,I Holm,R Hopkin,W Introne,M Lyons,D Monteil,A Scheuerle,J Stoler,S Vergano,Chen Hamid,R Downs,S Grout,R Cunniff,C Parisi,M Ralston,S Scott,J Shapira,S Spire,P (2022). Health Supervision for Children and Adolescents With Down Syndrome.
Maria Pelleri,Elena Gennari,Chiara Locatelli,Allison Piovesan,Maria Caracausi,Francesca Antonaros,Alessandro Rocca,Costanza Donati,Letizia Conti,Pierluigi Strippoli,Marco Seri,Lorenza Vitale,Guido Cocchi (2017). Genotype-phenotype correlation for congenital heart disease in Down syndrome through analysis of partial trisomy 21 cases.
Pasqualina Picciotti,Angelo Carfì,Roberta Anzivino,Gaetano Paludetti,Guido Conti,Vincenzo Brandi,Roberto Bernabei,Graziano Onder (2017). Audiologic Assessment in Adults With Down Syndrome.
M Channell,L Mattie,D Hamilton,G Capone,E Mahone,S Sherman,T Rosser,R Reeves,L Kalb,Down Syndrome,Cognition Project (2021). Capturing cognitive and behavioral variability among individuals with Down syndrome: a latent profile analysis.
Mary Chadi,Guy Saint Georges,Francine Albert,Gisele Mainville,Julie Nguyen,Adel Kauzman (2017). Major salivary gland aplasia and hypoplasia in Down syndrome: review of the literature and report of a case.
Yasas Jayaratne,Ibrahim Elsharkawi,Eric Macklin,Lauren Voelz,Gil Weintraub,Dennis Rosen,Brian Skotko (2017). The facial morphology in Down syndrome: A 3D comparison of patients with and without obstructive sleep apnea.
Daniel Klingel,Ariane Hohoff,Robert Kwiecien,Dirk Wiechmann,Thomas Stamm (2017). Growth of the hard palate in infants with Down syndrome compared with healthy infants—A retrospective case control study.
Christophe Maïano,Olivier Hue,Geneviève Lepage,Alexandre Morin,Danielle Tracey,Grégory Moullec (2019). Do Exercise Interventions Improve Balance for Children and Adolescents With Down Syndrome? A Systematic Review.
A Carfì,R Liperoti,D Fusco,S Giovannini,V Brandi,D Vetrano (2017). Bone mineral density in adults with Down Syndrome.
C Cua,U Haque,Y Miao,C Backes (2017). Necrotizing Enterocolitis Incidence, characteristics, and Outcomes in Neonatal Down Syndrome Patients.
Beatriz Bermudez,Sandra Medeiros,Mariane Bermudez,Iolanda Novadzki,Neiva Magdalena (2015). Down syndrome: Prevalence and distribution of congenital heart disease in Brazil.
Maurice Beghetti,Andrzej Rudzinski,Min Zhang (2017). Efficacy and safety of oral sildenafil in children with Down syndrome and pulmonary hypertension.
M García-Hoyos,J Riancho,C Valero (2017). Bone health in Down syndrome.
Roba Elrefadi,Hawwa Beaayou,Khadiga Herwis,Ahmed Musrati (2022). Oral health status in individuals with Down syndrome.
Cofd Amaral,F Straioto,M Napimoga,E Martinez (2017). Caries experience and salivary aspects in individuals with fragile X syndrome.
Renata Cabral,Leandro Hilgert,Jorge Faber,Soraya Leal (2014). Caries risk assessment in schoolchildren - a form based on Cariogram® software.
Cristhiane Do Amaral,Kamila Kantovitiz,V De Araújo,T Marega,L Teixeira,E Martinez (2024). Assessment of dental and periodontal indices and <scp><i>Streptococcus mutans</i></scp> virulence in fragile X syndrome patients.
R Team (2020). R: A Language and Environment for Statistical Computing.
F Mohd,A Said,M Ismail (2022). Two Case Reports of Intravenous Midazolam Sedation in Patients with Down Syndrome Receiving Dental Treatment.
Cristhiane Amaral,Luana Pereira,Nayara Guy,Marcelo Amaral Filho,Gustavo Logar,Fabiana Straioto (2016). Oral health evaluation of cardiac patients admitted to cardiovascular pre-surgery intervention.
A Rexhepi,V Hamiti,Z Agani,T Kutllovci,B Xhemajli,M Loxha (2019). Efficacy of Antibiotic Prophylaxis in The Prevention of Bacterial Endocarditis in Dental Practice.
C Areias,B Sampaio-Maia,H Guimaraes,P Melo,D Andrade (2011). Caries in Portuguese children with Down syndrome.
Tahyna Deps,Gabriela Angelo,Carolina Martins,Saul Paiva,Isabela Pordeus,Ana Borges-Oliveira (2015). Association between Dental Caries and Down Syndrome: A Systematic Review and Meta-Analysis.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Cristhiane Amaral. 2026. \u201cDown Syndrome – Trisomy of Chromosome 21: Medical Considerations, Physiological, and Oral Health Perspectives\u201d. Global Journal of Medical Research - J: Dentistry & Otolaryngology GJMR-J Volume 24 (GJMR Volume 24 Issue J1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.