Acute kidney injury (AKI) is one of the main secondary manifestations developed in patients with COVID-19. Based on this aspect, the present study aimed to identify the main biomarkers used to predict acute kidney injury and prognosis in COVID-19 and gather information about the biomarkers studied. Articles published in the Virtual Health Library, between January 2020 and February 2022, in English, Portuguese and Spanish were evaluated, with the guiding question “What is the scientific evidence on new biomarkers for diagnosis and determination of the prognosis of induced acute kidney injury?” in COVID-19?”. Initially, more than 75 thousand articles were identified, however, with the attribution of inclusion and exclusion criteria, 8 articles were selected and analyzed during the present study. The findings of the present review emphasize that early diagnosis has a strong influence on the prognosis of AKI and that new biomarkers are useful for detecting and predicting the prognosis of the injury early. The potential of these assays with new biomarkers proved to be significant and could allow their use in future research.
## I. INTRODUCTION
During the COVID-19 pandemic, part of the individuals infected with SARS-CoV-2 manifested a mild to moderate respiratory illness, however, many elderly people and people with other comorbidities evolved to severe conditions[^1]. Patients in the intensive care unit (ICU) developed secondary complications, such as liver damage, venous thromboembolism, acute kidney injury (AKI), and others[^2]. AKI in this case is correlated with poor prognosis and a higher risk of patient mortality[^3].
Currently, the definition and staging of acute kidney injury are based on the KIDGO (Kidney Disease Improving Global Outcomes) criteria, which unifies the RIFLE (Risk, Injury, Failure, Loss and End-Stage) and AKIN (Acute Kidney Injury Network) criteria. Thus, KDIGO uses changes in serum creatinine and urinary output, requiring at least two serum creatinine values obtained in 48 hours[^5].
Serum creatinine levels increase as a $50\%$ drop in renal function occurs, that is, it is not directly correlated with the decrease in glomerular filtration rate (GFR), which makes early diagnosis impossible. Given this, in recent years, studies with new biomarkers for AKI have gained emphasis in different clinical settings. Among the new biomarkers tested are: Cystatin C, Lipocalin Associated with Human Neutrophil Gelatinase (NGAL), N-acetyl -B-D-glucosaminidase (NAG), Kidney Injury Molecule-1 (KIM-1), Interleukin-18 (IL -18), Netrin-1 and others[7,8].
Given the difficulty of diagnosing AKI using serum creatinine and the inefficient prognosis in COVID-19, the use of biomarkers such as Cystatin C and interleukin-18 is suggested[^9]. Cystatin C is a cysteine proteinase inhibitor protein, which is related to several pathological processes. It is freely filtered in the glomeruli, as it has a low molecular weight, but is almost completely reabsorbed in the proximal tubules[^10]. Interleukin-18 is a pro-inflammatory cytokine that induces the release of inflammatory cytokines and TNF, thus acting as a mediator in the immune system[^6].
The present work is a systematic review of the comprehensive literature, with the main objective of exploring biomarkers for the early diagnosis of AKI induced by COVID-19. Predicting and/or determining the patient's prognosis, as this is of clinical importance and is extremely necessary to apply as a laboratory practice.
## II. METHODS
### a) Instrument for selection of studies and inclusion criteria
The instrument for selecting the studies was the Relevance Test (TR), based on Pereira's model (2006)[^11]. This consists of forms containing four selection steps, to include or exclude the articles found with the search strategy.
Initially, TR1 was applied to the references to select studies that meet the following inclusion criteria:
- Publications made from January 2020 to February 2022;
- Published in Portuguese, English and Spanish.
As exclusion criteria, those who did not meet the criteria described above were considered.
### b) Definition of descriptors and search in the literature
A literature search was performed by crossing the following descriptors in Health Sciences/Medical Subject Headings (DeCS/MeSH) available on the VHL network: Acute Kidney Injury and COVID-19 "OR" SARS-CoV- two. The articles were searched using the advanced method, using the term "title/abstract/subject" with the combination of descriptors and the Boolean operators "AND" and "OR".
### c) Data extraction and analysis
Taking into account the methodological rigor of a systematic literature review (SLR), a form was prepared to extract the following information from the included studies: bibliographic reference, type of study, research objectives, methodology, and results obtained[^12]. To synthesize as much information as possible about the biomarkers for the prognosis of AKI, the following data were collected: characteristics and clinical conditions of the patients, criteria for diagnosing AKI, biomarkers used, the value of the biomarker and serum creatinine on admission and whether there was any change in the glomerular filtration rate (GFR), biomarker performance for AKI prognosis and clinical outcomes.
## III. RESULTS
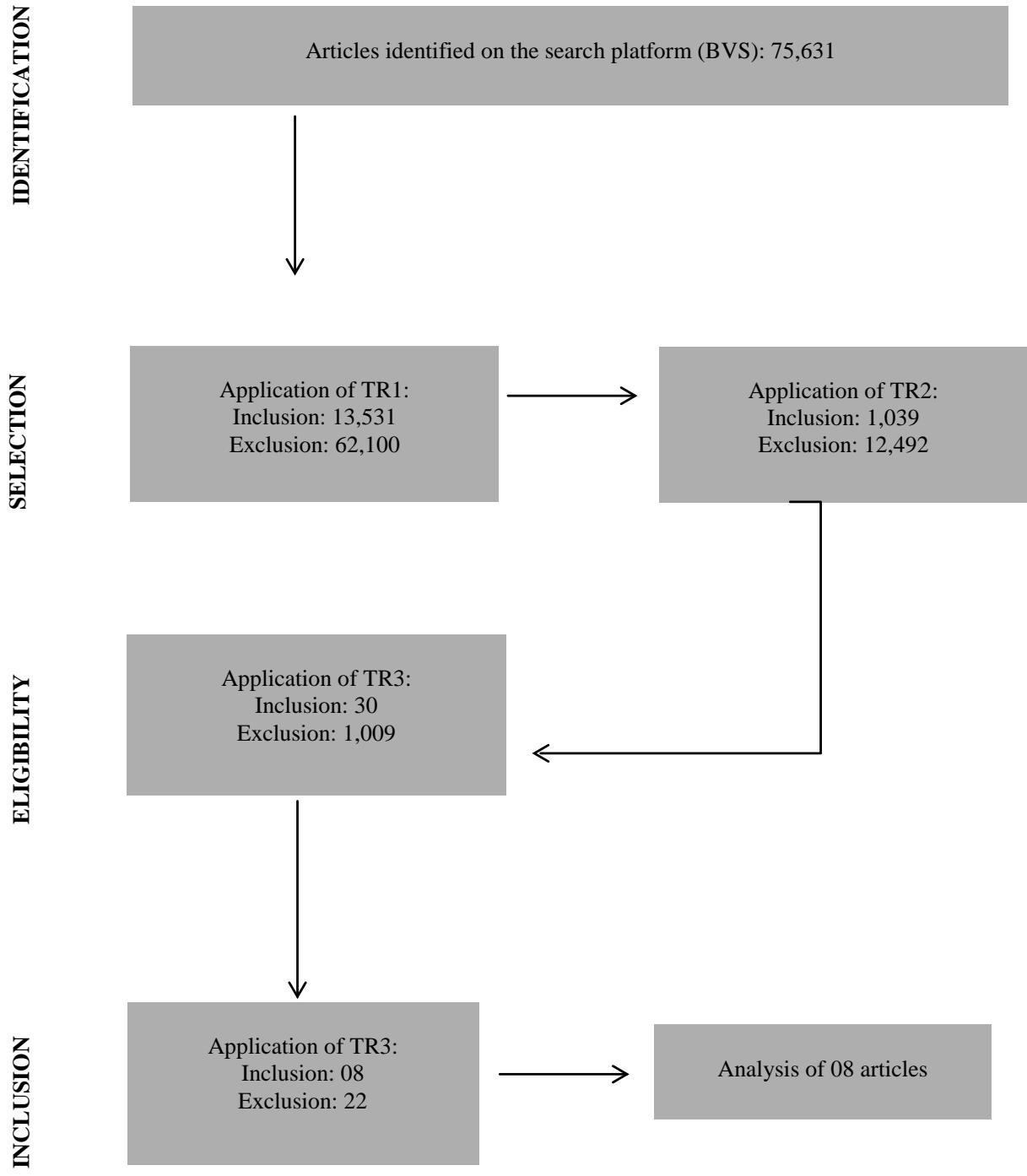
Bearing in mind that new articles are inserted in the databases every day, April 24, 2022, was chosen to carry out the bibliographic research of this RSL. A total of 75,631 articles were obtained, of which TR1 was applied. After applying the first test, a total of 13,531 articles were included, in which the TR2 was applied in the titles and abstracts with the help of the search platform, 12,492 studies were excluded and 1,039 were included. In the next step, TR3 was applied to the abstracts of previously selected articles, which resulted
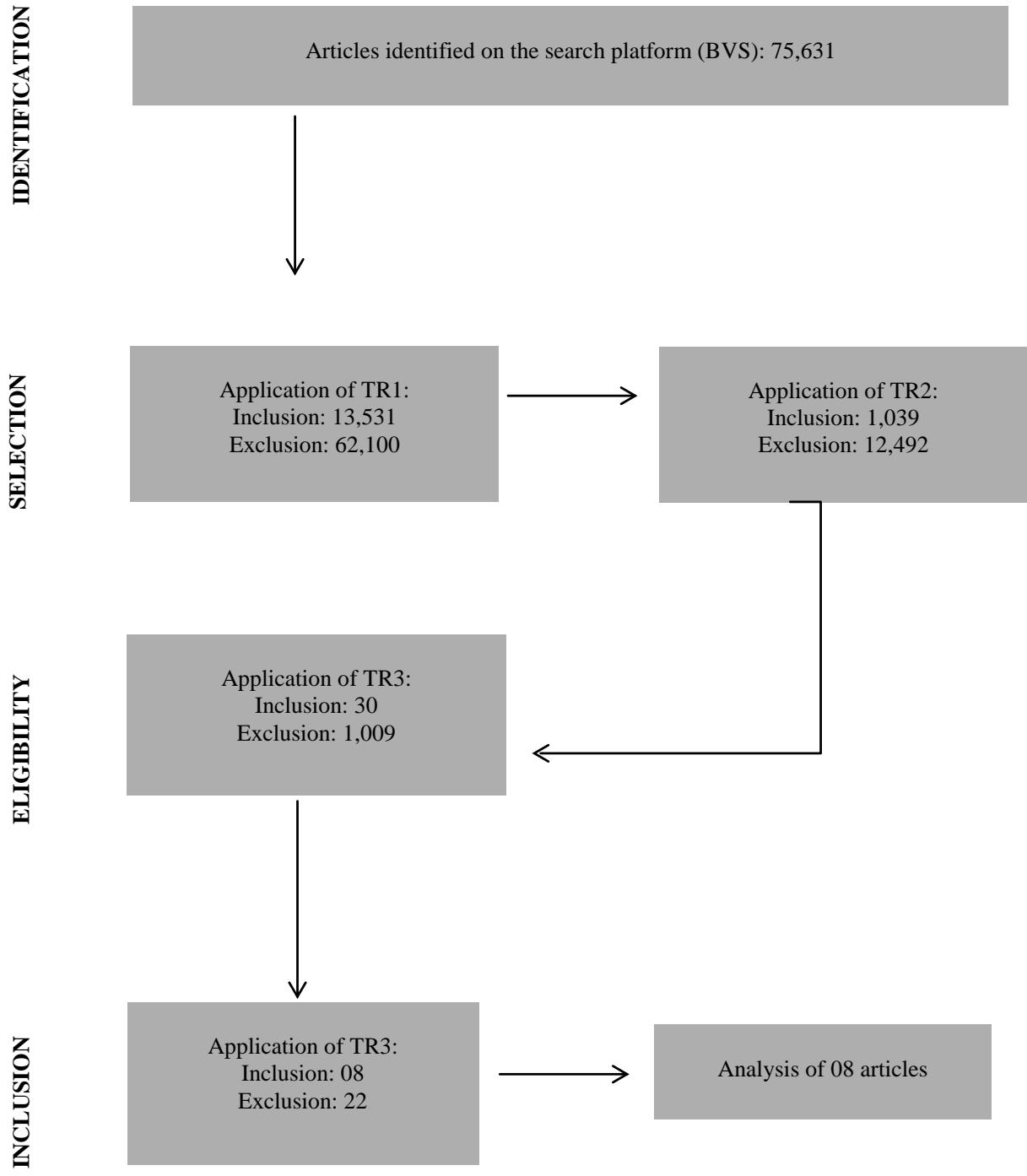 Figure 1: Methodological approach used in the Systematic Review of the Literature on biomarkers for the prognosis of acute kidney injury induced by COVID-19 (BVS, 2022).
After analyzing the eight studies selected for this SLR, a summary of the general characteristics was prepared and made available in synoptic tables. In Frame 1, information and characteristics of the articles analyzed during the study are presented.
Frame 1: Information and characteristics of the articles selected during the study
<table><tr><td>Reference</td><td>Study design</td><td>Selection of participants</td></tr><tr><td>Temiz et al. (2022)</td><td>A prospective pilot study</td><td>Participants were selected from the urology and ICU departments suspected, suspected of COVID-19 and with specific findings on tomography</td></tr><tr><td>Shakked et al. (2022)</td><td>Prospective observational investigation</td><td>Adults (≥18 years) and patients who test positive for Covid-19</td></tr><tr><td>Husain-Syed et al. (2021)</td><td>Prospective, observational, single-centre study</td><td>Patients were included if they consented to the linkage with administrative data for longterm follow-up</td></tr><tr><td>Gradin et al. (2021)</td><td>Study is a sub-study of a larger prospective observational</td><td>Adult patients with COVID-19 admitted to the ICU and with informed consent, in addition to urinary samples included in the study</td></tr><tr><td>Vogel et al. (2021)</td><td>Cohort of COVID-19 patients in this prospective observational clinical trial</td><td>Patients presenting with acute symptoms of respiratory infection. The secondary outcome was a composite of acute kidney injury, ICU admission, and death</td></tr><tr><td>Indirli et al. (2022)</td><td>A single-centre, observational, retrospective, case-control study</td><td>Data were retrospectively extracted from the COVID-19 Network registry</td></tr><tr><td>Fukao et al. (2021)</td><td>Retrospective study</td><td>Used data from all patients with COVID-19 seen</td></tr><tr><td>Wang et al. (2021)</td><td>Prospective observational investigation</td><td>Patients admitted to for COVID- 19, were eligible for this study</td></tr></table>
Biomarker predictors of poor prognosis such as ICU stay, renal replacement therapy (RRT), or death were observed for patients with AKI in COVID-19, as shown in Frame 2.
Frame 2: Prognostic predictor biomarkers for AKI in COVID-19
<table><tr><td>Reference</td><td>Biomarker</td><td>Prognosis</td></tr><tr><td>Temiz et al. (2022)</td><td>KIM-1/creatinine and NGAL/creatinine</td><td>Death</td></tr><tr><td>Shakked et al. (2022)</td><td>Serum creatinine
Serum cystatin C and NGAL</td><td>AKI
AKI aggravation
RRT needs
Admission in ICU</td></tr><tr><td>Husain-Syed et al. (2021)</td><td>Urinary DKK33</td><td>AKI Chronification</td></tr><tr><td>Gradin et al. (2021)</td><td>Serum creatinine
Urinary KIM-1
Urinary NGAL</td><td>Correlation with urinary cytokines
AKI aggravation</td></tr><tr><td>Vogel et al. (2021)</td><td>Serum creatinine
urinary KIM-1
urinary NAG</td><td>AKI, ICU e Death</td></tr><tr><td>Indirli et al. (2022)</td><td>MR – Serum ProADM
serum copeptin</td><td>Sepsis and AKI;
Death, ICU or
Hospital complications.</td></tr></table>
DKK33 Dickkopf-related protein 3, KIM-1 Kidney Injury Molecule 1, AKI Acute Kidney Injury, NAG N-acetyl-β-D-glucosaminidase, NGAL Neutrophil gelatinase-associated lipocalin, MR - ProADM Mid-regional pro-adrenomedullin, TRS Therapy Renal replacement, ICU Intensive care unit.
Two studies evaluated biomarkers that were useful for early diagnosis, these markers are shown in Frame 3.
Frame 3: Biomarkers for early diagnosis
<table><tr><td>Reference</td><td>Biomarker</td></tr><tr><td>FUKAO et al. (2021)</td><td>L-FABP and urinary β2MG</td></tr><tr><td>WANG et al. (2021)</td><td>Serum procalcitonin (PCT)</td></tr></table>
$\beta 2MG$ $\beta 2$ -microglobulin, L-FABP Liver-type fatty acid binding protein.
When analyzing the characteristics of the clinical conditions of the populations of the eight studies, it was observed that among the eight studies, the size of the population with COVID-19 ranged from 18 to 389 patients, with three studies presenting, in addition to the COVID-19 cohort, a control group, such as can be observed in Table 1.
<table><tr><td>Reference</td><td>Sample No.</td><td>AKI (%)</td><td>Age (average or median + IQ)</td><td>Comorbidities</td></tr><tr><td>Temiz et al. (2022)</td><td>75 COVID-19 11 Control</td><td>16</td><td>55,77 ± 17,47</td><td>Hypertension</td></tr><tr><td>Shakked et al. (2022)</td><td>52</td><td>42,3</td><td>66</td><td>Heart failure, hypertension, chronic kidney disease, cerebrovascular disease</td></tr><tr><td>Husain-Syed et al. (2021)</td><td>55</td><td>10,45</td><td>54</td><td>Hypertension, diabetes, chronic kidney disease, coronary artery disease</td></tr><tr><td>Gradin et al. (2021)</td><td>29 COVID-19 9 Control</td><td>66</td><td>57 ± 3</td><td>Hypertension, chronic lung disease, and diabetes mellitus</td></tr><tr><td>Vogel et al (2021)</td><td>54 COVID-19 26 Control</td><td>14,8</td><td>56,8</td><td>Hypertension, chronic lung disease, and diabetes mellitus</td></tr><tr><td>Indirli et al. (2022)</td><td>116</td><td>3</td><td>66</td><td>Hypertension, diabetes, obesity, and coronary artery disease</td></tr><tr><td>Fukao et al. (2021)</td><td>18</td><td>11</td><td>64,0 (44,0–74,5)</td><td>Hypertension, diabetes mellitus, and coronary heart disease</td></tr><tr><td>Wang et al. (2021)</td><td>389</td><td>7,8</td><td>66 (15)</td><td>Hypertension diabetes mellitus, liver disease</td></tr></table>
<table><tr><td>Reference</td><td>Sample No.</td><td>AKI (%)</td><td>Age (average or median + IQ)</td><td>Comorbidities</td></tr><tr><td>Temiz et al. (2022)</td><td>75 COVID-19 11 Control</td><td>16</td><td>55,77 ± 17,47</td><td>Hypertension</td></tr><tr><td>Shakked et al. (2022)</td><td>52</td><td>42,3</td><td>66</td><td>Heart failure, hypertension, chronic kidney disease, cerebrovascular disease</td></tr><tr><td>Husain-Syed et al. (2021)</td><td>55</td><td>10,45</td><td>54</td><td>Hypertension, diabetes, chronic kidney disease, coronary artery disease</td></tr><tr><td>Gradin et al. (2021)</td><td>29 COVID-19 9 Control</td><td>66</td><td>57 ± 3</td><td>Hypertension, chronic lung disease, and diabetes mellitus</td></tr><tr><td>Vogel et al (2021)</td><td>54 COVID-19 26 Control</td><td>14,8</td><td>56,8</td><td>Hypertension, chronic lung disease, and diabetes mellitus</td></tr><tr><td>Indirli et al. (2022)</td><td>116</td><td>3</td><td>66</td><td>Hypertension, diabetes, obesity, and coronary artery disease</td></tr><tr><td>Fukao et al. (2021)</td><td>18</td><td>11</td><td>64,0 (44,0–74,5)</td><td>Hypertension, diabetes mellitus, and coronary heart disease</td></tr><tr><td>Wang et al. (2021)</td><td>389</td><td>7,8</td><td>66 (15)</td><td>Hypertension diabetes mellitus, liver disease</td></tr></table>
Frame 4: General characteristics of studies with biomarkers for prognosis
<table><tr><td>Reference</td><td>Type of study</td><td>Objectives</td><td>Methodology</td><td>Conclusions</td></tr><tr><td>Temiz et al. (2022).</td><td>Prospective pilot</td><td>Investigate whether there is kidney damage during COVID-19; Identify the predictive value of renal biomarkers and estimate survival.</td><td>KIM-1/creatinine and NGAL/creatinine ratios were compared among 36 patients with COVID-19 and 11 controls. Mortality rates were determined using the Kaplan-Meier method.</td><td>Urine KIM-1/creatinine ratio associated AKI with COVID-19-specific death. In clinical practice, serum Cystatin C (sCysC) and urine KIM-1/creatinine are associated with survival.</td></tr><tr><td>Shakked et al. (2022).</td><td>Prospective, observational</td><td>To evaluate the usefulness of serum CysC (sCysC) and serum NGAL (sNGAL).</td><td>Demographic data of 52 patients were retrieved from medical records. sCysC, serum creatinine, and serum and urine NGAL were analyzed.</td><td>sCysC was an excellent early predictor of AKI and the need for RRT in patients with COVID-19, but it did not outperform serum creatinine. While sNGAL showed good performance for the diagnosis of AKI.</td></tr><tr><td>Husain-Syed et al. (2021).</td><td>Prospective, observational</td><td>Evaluate the role of renal biomarkers to monitor the progression of COVID-19.</td><td>Spot urine samples were collected from 55 patients daily and for analysis of uDKK3 and IL-6 it was collected three times a week from hospital admission until the day of discharge.</td><td>Biphasic patterns of urinary uDKK3 and IL-6 in patients with a greater decrease in eGFR are suggestive of a chronification of AKI and commonly used urinary markers may be less suitable.</td></tr></table>
Fukao et al. (2021).
<table><tr><td>Reference</td><td>Type of study</td><td>Objectives</td><td>Methodology</td><td>Conclusions</td></tr><tr><td>Fukao et al. (2021).</td><td>Prospective observational clinical trial</td><td>Investigate relationships of tubular injury, COVID-19 severity, and markers of inflammation To address cytokine-mediated mechanisms in the development of AKI.</td><td>Analysis of markers and respiratory status was performed in 18 patients with COVID-19. Correlation analysis among levels of tubular and laboratory markers.</td><td>Urinary markers L-FABP and uβ2MG were significantly associated with IL-6 levels even in patients without overt AKI. It is suggested that L-FABP and urinary uβ2MG are useful as early diagnostic biomarkers.</td></tr><tr><td>Wang et al. (2021).</td><td>Exploratory</td><td>To assess the value of PCT in predicting AKI during COVID-19. Build a risk classification score.</td><td>The biomarker concentrations of 28 patients with COVID-19 were analyzed. A multivariate risk score was created.</td><td>Single PCT value is a valuable predictive marker of AKI in patients with COVID-19. The risk score can help assess the possibility of developing AKI.</td></tr></table>
β2MG β2-microglobulin, IL-6 Interleucina 6, L-FABP Liver-type fatty acid binding protein, AKI Acute kidney injury, PCT Procalcitonin.
After analyzing the studies, it is observed that the classification used for the detection of AKI was KDIGO (2012), having been used in seven of the eight studies found, and only one study did not present this information. Biomarkers were analyzed in blood and urine samples, with analysis of serum biomarkers being the most prevalent among the eight studies. The dosage of these markers was carried out from the moment of consultation in the emergency department or hospital admission. In summary, this information is available in Frames 6 and 7.
Frame 6: Biomarkers for AKI prognosis in patients with COVID-19.
<table><tr><td>Reference</td><td>Biomarker</td><td>Serum or urinary</td><td>Biomarker value on admission (median ± IQR)</td><td>Biomarker performance for early diagnosis and prognosis</td></tr><tr><td rowspan="5">Temiz et al. (2022)</td><td>Creatinine</td><td>Serum</td><td>0,75 +/- 0,39 (mg/dL)</td><td>Elevated KIM-1/creatinine: death from COVID-19.</td></tr><tr><td>Cystatin C</td><td>Serum</td><td>0,96 +/- 0,59 (mg/L)</td><td>Higher elevation</td></tr><tr><td rowspan="2">Fukao et al. (2021)</td><td>NAG</td><td>Urinary</td><td>32,5 U/L</td><td>There was no correlation.</td></tr><tr><td>β2MG</td><td>Urinary</td><td>10.516 μg/L</td><td>Elevations in L-FABP and uβ2MG</td></tr><tr><td rowspan="3"></td><td>Uric acid</td><td>Serum</td><td>408 (235-670) (umol/L)</td><td>Decrease in GFR</td></tr></table>
AUC Area under the curve, $\alpha 1MGCR$ $\alpha 1$ -microglobulin-creatinine ratios, CKD Chronic kidney disease, eGFR Estimated glomerular filtration rate, KIM-1 Kidney Injury Molecule 1, MR - ProADM Mid-regional pro-adrenomedullin, NAG N-acetil- $\beta$ D-glicosaminidase, NGAL Neutrophil gelatinase-associated lipocalin, AKI Acute kidney injury, GFR Glomerular filtration rate, RRT Renal replacement therapy, uα1MG Urinary α1 microglobulin, uDKK3 Urinary Dickkopf-3, ICU Intensive care unit.
$\alpha 1MG \alpha 1$ microglobulin, $\beta 2MG \beta 2$ -microglobulin, L-FABP Liver-type fatty acid binding protein AKI Acute kidney injury, NAG N-acetil- $\beta$ -D-glicosaminidase, PCT Procalcitonin, GFR Glomerular filtration rate.
Regarding the results for prognosis, it was seen that the biomarkers used were predictors of poor prognosis. KIM-1/creatinine and NGAL/creatinine ratios were predictors of death from COVID-19 $^{13}$. Serum creatinine and cystatin C were indicators of AKI, worsening of the lesion, and need for RRT. The NAG marker was significant for predicting AKI in patients with severe AKI who required RRT $^{14}$. Elevation in the urinary biomarker uDKK33 at six months from hospital admission was suggestive of AKI chronicity by COVID-19 $^{15}$. Serum creatinine and urinary biomarkers KIM-1 and NGAL correlated with urinary cytokines of incidence and worsening of AKI $^{16}$. Serum creatinine and KIM-1 were significantly elevated in patients who achieved the composite endpoint (acute kidney injury, ICU, and death) and the NAG marker was significantly elevated in patients who suffered from AKI $^{17}$.
In Frame 7, the results of two studies with biomarkers for the early diagnosis of AKI in COVID-19 are available.
## IV. DISCUSSION
The electronic survey involved studies carried out during the COVID-19 pandemic, published between 2021 and 2022. Given the pandemic context, one can observe agility in carrying out the surveys. In addition, according to the analyzed studies, it is observed that the search for new AKI laboratory biomarkers for the identification and progression of AKI continues to advance.
Despite the size of the sample (18 to 389 participants), no influence was verified on the characteristics and clinical conditions of the patients. It was observed that among the eight studies, the patients who developed AKI were over 50 years old, and were hypertensive or diabetic. In addition, the KDIGO diagnostic criteria, GFR calculation using the CKD-EPI formula, and biomarker analysis (ELISA) were also similar among studies. In addition to this, nephelometric tests were also used, mainly to analyze Cystatin C, which helps in the comparison between them. Although unusual, Cystatin C is considered an early marker of AKI and its dosage has been performed with nephelometric tests, as they are considered quite stable $^{18}$.
Among the biomarkers, urinary KIM-1 stood out as the most promising for the diagnosis and prognosis of AKI. Significant elevations were found in the KIM-1/urinary creatinine ratio in patients with AKI and specific deaths from COVID-19 $^{13}$. Consistently, a significant increase in KIM-1 levels between 24h and 48h after admission to the ICU in patients with septic AKI due to other diseases who did not survive was also verified $^{19}$. In a study by ${}^{16}$, a correlation of urinary KIM-1 with several urinary cytokines related to the incidence and worsening of AKI in COVID-19 was observed. The results of ${}^{17}$ showed elevations in urinary KIM-1 levels in COVID-19-positive patients with a composite outcome of AKI, ICU admission, and death. Similarly, in a study carried out with patients hospitalized with AKI in other diseases, the increase in urinary KIM-1 and NAG levels at the time of consultation with a nephrologist were predictors of the composite outcome of RRT or in-hospital death $^{20}$.
The second prominent biomarker was NGAL, both for serum concentrations and urinary levels. Serum NGAL was useful for predicting AKI, need for RRT, ICU stay, and expressly highs in severe AKI requiring RRT $^{14}$. NGAL/creatinine was useful as a good predictor of mortality in patients with COVID-19 and AKI $^{13}$. Similar results were found in a study with critically ill patients due to other diseases, where $40\%$ more cases of AKI were detected with the evaluation of NGAL and creatinine than when using creatinine alone, and in these patients, the risk of ICU admission, need for TRS and death was higher $^{21,22}$.
Another biomarker with prognostic results for AKI was sCysC, whose elevation exceeded the urinary KIM-1/creatinine and NGAL/creatinine ratio in ICU patients, but was not considered a predictor of specific mortality from COVID-19 $^{13}$. Serum and urine creatinine were used in all eight studies, as it is the standard AKI diagnostic marker. On admission, serum creatinine was similar to sCysC for predicting AKI and the need for
- $\mathsf{RRT}^{14}$. However, the elevation of sCysC compared to serum creatinine may have been influenced by high doses of corticosteroids[^15].
- In the analysis of urinary dickkopf-3 (uDKK3), a new biomarker of CKD progression. uDKK3 levels remained high 6 months after hospital admission for COVID-19 in patients with AKI and a greater decline in glomerular filtration. The existence of a secondary AKI over an unresolved AKI has been suggested, which may contribute to the transition from AKI to CKD at 6 months post-discharge15. These findings are similar to what is in the literature, since in a study with post-cardiac surgery patients, urinary DKK3 was associated with a risk of severe loss of glomerular filtration after the transition from AKI to CKD during the patients' follow-up period23.
- As for biomarkers for early diagnosis of AKI, the highlights were $\beta 2\mathrm{MG}$ and L-FABP, which were elevated in urine samples as a reflection of the onset of $\mathrm{AKI}^{24}$. L-FABP is a protein present in the liver that plays an important role in regulating the metabolism of fatty acids. In addition, it has a high affinity for lipid peroxidation products, which promotes its elimination in the urine[25].
- 26 Evaluated common biomarkers, but included serum PCT dosage in their study, which in turn was useful for early detection of AKI in patients with COVID-1927.
- Although the cost of testing may still be a limiting factor, the results have shown promise for assessing the incidence of AKI with new biomarkers $^{16,28,14,17}$, predict AKI severity, help identify patients who need RRT $^{16,14}$ or ICU $^{28,14,17}$, predict death $^{28,17,13}$ and perform early detection of AKI in COVID-19 $^{24,26}$, thus minimizing the cost of the test.
- With the use of new biomarkers detected before serum creatinine, it was possible to detail the AKI caused by COVID-19 for the first time in the literature[^13]. The evaluation of biomarkers such as KIM-1 and Cystatin C at admission can provide diagnostic data and help to outline the prognosis of AKI, which can influence medical decisions and thus increase the chances of better outcomes<sup>17,14</sup>. In addition, it is considered important to evaluate the renal system in COVID-19 with AKI biomarkers, as well as to consider their continuous evaluation during hospitalization[^13].
- The application of new sensitive biomarkers for AKI proved to be important for the diagnosis and prognosis of the lesion in the COVID-19 scenario.
- Different biomarkers were able to predict AKI severity, need for RRT, hospitalization, and death. The poor prognosis of AKI in COVID-19 observed in the analyzed studies highlights the importance of identifying new biomarkers and applying them in laboratory practice and different clinical scenarios.
- Although the use of some of these biomarkers is limited due to the high cost of the necessary reagents,
Disclosure statement
- No potential conflict of interest was reported by the author(s).
Funding
Generating HTML Viewer...
References
28 Cites in Article
(2021). WHO-Convened Global Study of Origins of SARS-CoV-2: China Part (Text Extract).
J Nicholas,E Tom,F Robert (2021). Doença do coronavírus 2019 (COVID-19).
Loami Martins (2020). Ocorrência de injúria renal aguda em pacientes internados por COVID-19 em um hospital público universitário em São Paulo, Brasil.
T Levi,Souza Sp De,J Magalhães,De,Carvalho Ms De,Alb Cunha,Jgao Dantas (2013). Comparação dos critérios RIFLE, AKIN e KDIGO para predizer mortalidade em pacientes críticos.
José Lopes,Sofia Jorge (2013). The RIFLE and AKIN classifications for acute kidney injury: a critical and comprehensive review.
E Macedo (2011). Biomarcadores na injuria renal aguda.
Luis Peres,Ademar Cunha Júnior,Alex Schäfer,Aline Silva,Arianne Gaspar,Deborah Scarpari,Julia Alves,Rodolfo Girelli Neto,Thaís Oliveira (2013). Biomarkers of acute kidney injury.
Kianoush Kashani,Wisit Cheungpasitporn,Claudio Ronco (2017). Biomarkers of acute kidney injury: the pathway from discovery to clinical adoption.
Y Koza (2016). Acute kidney injury: Current concepts and new insights.
Thelma Okay,C Cistatina (2002). Cistatina C: um novo marcador de função renal em crianças.
A Pereira (2006). Revisão sistemática da literatura sobre produtos usados tratamento de feridas.
L Carneiro,J Paula,J Aguiar,P Ludvig (2017). CONCRETO AUTOCICATRIZANTE PELA INTRODUÇÃO DE BACTÉRIAS – UMA REVISÃO.
Mustafa Temiz,Ibrahim Hacibey,Ramazan Yazar,Mehmet Sevdi,Suat Kucuk,Gizem Alkurt,Levent Doganay,Gizem Dinler Doganay,Muhammet Dincer,Emrah Yuruk,Kerem Erkalp,Ahmet Muslumanoglu (2022). Altered kidney function induced by SARS-CoV-2 infection and acute kidney damage markers predict survival outcomes of COVID-19 patients: a prospective pilot study.
N Shakked,Oliveira Mhs De,I Cheruiyot,J Benoit,M Plebani,G Lippi (2022). Early prediction of COVID-19-associated acute kidney injury: Are serum NGAL and serum Cystatin C levels better than serum creatinine?.
S Silva,Da (2020). O papel dos biomarcadores TIMP-2, IGFBP7 e L-FABP no diagnóstico da lesão renal aguda.
R Wang,M He,Y Kang (2021). A risk score based on procalcitonin for predicting acute kidney injury in COVID-19 patients.
Silva Mr Castro Mc De,Da (2012). Procalcitonina no diagnóstico de doenças infecciosas.
R Indirli,A Bandera,L Valenti,F Ceriotti,A Modugno,M Tettamanti (2022). Prognostic value of copeptin and mid-regional proadrenomedullin in COVID-19-hospitalized patients.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Venine Prado Saêta. 2026. \u201cExploring Biomarkers for Early Prognosis of COVID-19-Induced Acute Kidney Injury: A Comprehensive Systematic Review\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 24 (GJMR Volume 24 Issue F1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.