

I. INTRODUCTION
Rectal cancer remains a formidable healthcare challenge worldwide , characterized by its potential for local invasion, lymphatic spread, and distant metastasis. Accurate pre-operative staging is imperative for guiding treatment decisions, including the selection of appropriate neoadjuvant therapies , surgical approaches, and postoperative management strategies. Pre-operative staging not only informs clinicians about the extent of disease but also serves as a crucial prognostic indicator, guiding therapeutic interventions and facilitating patient counseling.
Traditionally, staging modalities for rectal cancer have included digital rectal examination, endorectal ultrasound (ERUS), and computed tomography (CT) imaging. However, these modalities have limitations in accurately assessing tumor extent, particularly in defining the relationship between the primary tumor and adjacent structures, as well as in detecting small lymph node metastases and distant metastatic disease. In recent years, advancements in imaging technology have led to the emergence of two pivotal modalities for pre-operative staging of rectal cancer: Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (F-FDG PET/CT) and magnetic resonance imaging (MRI) .
F-FDG PET/CT combines metabolic information from PET with anatomical details from CT, offering comprehensive insights into tumor metabolism, proliferation, and metastatic spread. The uptake of FDG, a glucose analog, reflects increased metabolic activity within malignant tissues, enabling the detection of distant metastases, particularly in the liver, lungs, and bones. Moreover, F-FDG PET/CT has shown promising results in assessing treatment response and predicting outcomes in rectal cancer patients undergoing neoadjuvant therapy.
In contrast, offers superior soft tissue contrast and multiplanar imaging capabilities, making it an invaluable tool for delineating tumor extent, assessing local invasion, and characterizing pelvic anatomy. High-resolution MRI sequences, such as T2-weighted imaging, diffusion-weighted imaging (DWI), and dynamic contrast-enhanced imaging, provide detailed anatomical information and enable accurate assessment of tumor stage, mesorectal fascia involvement, and nodal status. Additionally, MRI is less susceptible to artifacts from bowel gas and metallic implants compared to CT imaging, enhancing its utility in rectal cancer staging.
While both F-FDG PET/CT and MRI offer unique advantages in pre-operative staging of rectal cancer, comparative studies evaluating their diagnostic performance in a real-world clinical setting are limited.
Existing evidence suggests that these modalities may have complementary roles, with F-FDG PET/CT excelling in detecting distant metastases and MRI providing detailed information on local tumor characteristics and nodal involvement. However, discrepancies in sensitivity, specificity, and overall diagnostic accuracy between the two modalities necessitate further investigation to elucidate their respective roles and optimize staging strategies in rectal cancer patients.
Against this backdrop, this cross-sectional study aims to comprehensively compare the diagnostic performance of F-FDG PET/CT and MRI in pre-operative staging of rectal cancer. By evaluating patients diagnosed with rectal cancer who underwent both imaging modalities, we seek to provide valuable insights into their relative efficacy and use, informing clinical practice and guiding future research endeavors.
II. METHODOLOGY
In this cross-sectional study, a total of seventy (70) known cases of rectal cancer were included whose baseline parameters are as shown in table 1. These patients were equally divided into group A and group B each containing thirty-five (35) patients. Group A underwent F-FDG PET/CT imaging and group B underwent MRI imaging.
Inclusion Criteria:
Patients of age 18 or older with histologically confirmed rectal cancer.
Patients who underwent both F-FDG PET/CT and MRI for preoperative staging within specific time frame and has the availability of complete imaging studies and medical records for analysis.
Willingness to provide informed consent for participation in the study.
Exclusion Criteria:
Patients with contraindications to MRI or F-FDG PET/CT, including severe claustrophobia, metal implants, or allergy to contrast agents.
Prior pelvic radiation therapy, which could potentially impact imaging interpretation and staging accuracy.
Incomplete imaging studies or patient noncompliance, such as inadequate bowel preparation or motion artifacts or unable to give informed consent.
Patients with a history of other malignancies, to minimize confounding factors related to previous treatments or concurrent cancers.
Pregnancy or breastfeeding women, as both F-FDG PET/CT and MRI involve radiation exposure or contrast administration.
| Parameter | Total (n=70) | F-FDG PET/CT Group (n=35) | MRI Group (n=35) |
| Age (years), Mean (±SD) | 60.5 (±8.3) | 61.2 (±7.9) | 59.8 (±8.7) |
| Sex (Male/Female), n (%) | |||
| - Male | 42 (60%) | 20 (57.1%) | 22 (62.9%) |
| - Female | 28 (40%) | 15 (42.9%) | 13 (37.1%) |
| Tumor Location, n (%) | |||
| - Rectosigmoid | 20 (28.6%) | 10 (28.6%) | 10 (28.6%) |
| - Rectum | 50 (71.4%) | 25 (71.4%) | 25 (71.4%) |
| Tumor Size (cm), Mean (±SD) | 4.7 (±1.2) | 4.5 (±1.1) | 4.9 (±1.3) |
| Histological Subtype, n (%) | |||
| - Adenocarcinoma | 65 (92.9%) | 32 (91.4%) | 33 (94.3%) |
| - Mucinous carcinoma | 5 (7.1%) | 3 (8.6%) | 2 (5.7%) |
| Clinical T Stage (cT), n (%) | |||
| - T1 | 8 (11.4%) | 4 (11.4%) | 4 (11.4%) |
| - T2 | 15 (21.4%) | 7 (20%) | 8 (22.9%) |
| - T3 | 40 (57.1%) | 20 (57.1%) | 20 (57.1%) |
| - T4 | 7 (10%) | 4 (11.4%) | 3 (8.6%) |
| Clinical N Stage (cN), n (%) | |||
| - N0 | 38 (54.3%) | 18 (51.4%) | 20 (57.1%) |
| - N1 | 20 (28.6%) | 10 (28.6%) | 10 (28.6%) |
| - N2 | 12 (17.1%) | 7 (20%) | 5 (14.3%) |
The PET/CT examinations were conducted using synthesized 18F-FDG, with image acquisition 60 minutes post-injection. CT images were acquired with a multi-detector-row CT component covering the head to mid-thigh region. Reconstruction of PET images were performed using the 3D-OSEM method, with both conventional PET and PSF-PET reconstructions. The MRI examinations were carried out using either a 1.5-T or 3-T scanner, with imaging parameters varying based on the scanner used.
For imaging analysis, PET/CT scans were evaluated by consensus of two nuclear medicine physicians, with a focus on SUVmax and L/B ratio for lymph nodes. Meanwhile, MRI images were reviewed by two diagnostic radiologists, primarily focusing on lymph node evaluation and tumor invasion, particularly using high-resolution T2-weighted images and diffusion-weighted imaging (DWI). The staging findings from both imaging modalities were compared with histopathological analysis of the primary tumor and harvested lymph nodes.
Statistical analysis included sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy values for T and N staging, with comparisons made between conventional PET/CT, PSF-PET/CT, and MRI.
III. RESULTS
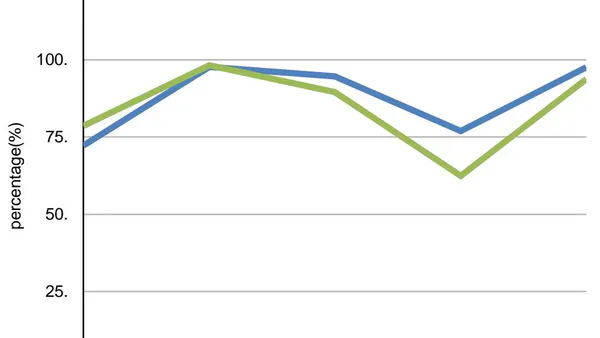
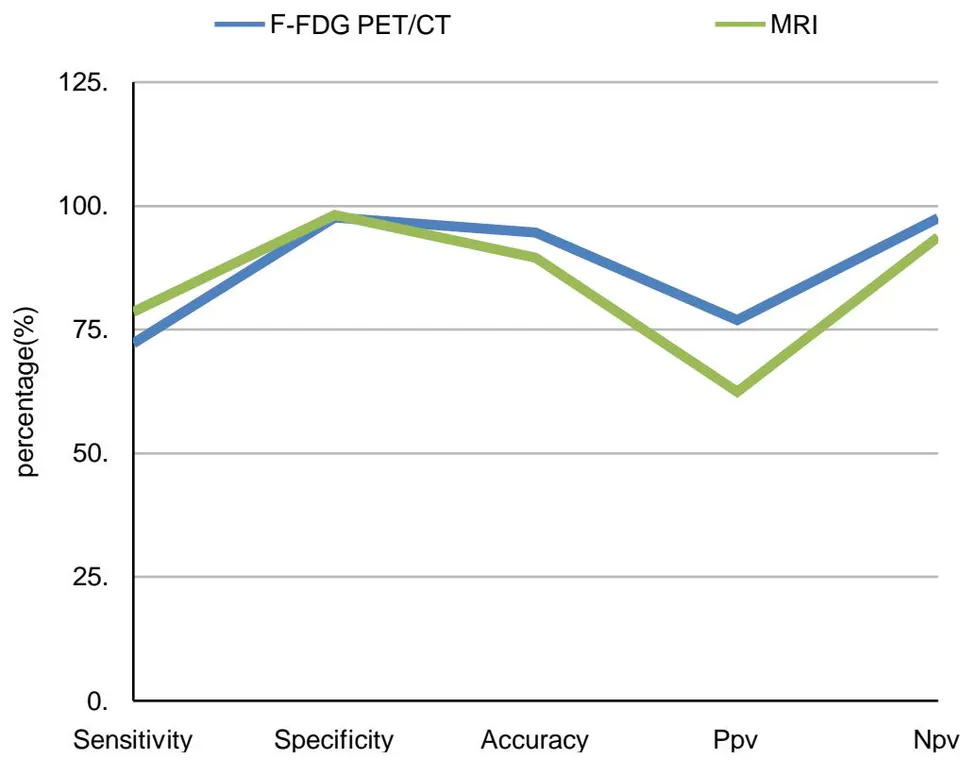
Preliminary analysis of seventy (70) patients in our study revealed that F-FDG PET/CT detected local tumor extent (table 2) and mesorectal fascia involvement with a sensitivity of [59.6], specificity of [94.8], PPV of [96.0], NPV of [52.7], and accuracy of [71.4]. MRI demonstrated a sensitivity of [72.0], specificity of [82.2], PPV of [90.8], NPV of [58.5], and accuracy of [75.5] for the assessment of local tumor extent. For assessing lymph node involvement (table 3 and figure 1), MRI exhibited a sensitivity of [78.6], specificity of [98.2], PPV of [62.5], NPV of [93.7], and accuracy of [89.6], compared to [72.2] sensitivity, [97.6] specificity, [76.9] PPV, [97.5] NPV, and [94.6] accuracy for F-FDG PET/CT. With regards to metastasis both F-FDG PET/CT detected all distant metastasis [9/70 patients; 3 cases for lung, 3 case for liver, 1 case for para-aortic LNs, and 2 case for lung, liver, and bone metas- tasis], whereas pelvic MRI was not able to diagnose distant metastases because of its scanning range limitations.
| F-FDG PET/CT | MRI | |
| Sensitivity% | 59.6 (0.49 to 0.79) | 72.0 (0.64 to 0.90) |
| Specificity% | 94.8 (0.76 to 0.98) | 82.2 (0.64 to.92) |
| Accuracy% | 71.4 (0.65 to 0.84) | 75.5 (0.69 to 0.87) |
| Ppv% | 96.0 (0.75 to 0.99) | 90.8 (0.76 to 0.99) |
| Npv% | 52.7 (0.43 to 0.82) | 58.5 (0.62 to 0.89) |
| Postive LR | 9.6 (2.43 to 72.60) | 5.7 (2.36 to 12.62) |
| Negative LR | 0.65 (0.54 to 0.76) | 0.58 (0.42 to 0.84) |
| F-FDG PET/CT | MRI | |
| Sensitivity | 72.2 | 78.6 |
| Specificity | 97.6 | 98.2 |
| Accuracy | 94.6 | 89.6 |
| Ppv | 76.9 | 62.5 |
| Npv | 97.5 | 93.7 |
| Positive LR | 19.6 | 10.9 |
| Negative LR | 0.46 | 0.68 |
The comparative evaluation of F-FDG PET/CT and MRI for preoperative staging of rectal cancer provides critical insights into the complementary nature of these imaging modalities. This study underscores the importance of utilizing both techniques to achieve a comprehensive understanding of disease extent, which is paramount for optimal patient management.
a) F-FDG PET/CT in Detecting Distant Metastases
F-FDG PET/CT has emerged as a powerful tool for detecting distant metastases due to its ability to highlight regions of increased glucose metabolism, which is a characteristic of many malignant cells. This capability is particularly advantageous in identifying metastases in organs such as the liver, lungs, and bones. The metabolic imaging provided by F-FDG PET/CT offers significant prognostic information that is crucial for patient stratification and treatment planning. Patients with detected distant metastases often require different therapeutic approaches compared to those with localized disease, making accurate detection vital for guiding treatment decisions.
However, the high sensitivity of F-FDG PET/CT can sometimes be a double-edged sword. The modality is prone to false positives, where benign processes such as inflammation or infection can exhibit increased glucose uptake, mimicking metastatic disease. This can lead to over-staging and potentially unnecessary treatments. Additionally, F-FDG PET/CT has limitations in detecting lesions that are either too small or have low metabolic activity, which can result in under-staging and missed metastatic sites. These limitations highlight the need for careful interpretation of F-FDG PET/CT results, considering the full clinical context and corroborating with other diagnostic findings.
b) MRI for Local Staging and Surgical Planning:
MRI is considered the gold standard for local staging of rectal cancer due to its superior soft tissue contrast and resolution. The high spatial resolution of MRI allows for detailed visualization of the primary tumor and its relationship with surrounding structures. Key aspects of local staging, such as tumor depth of invasion, involvement of the mesorectal fascia, and the presence of suspicious lymph nodes, can be assessed with high accuracy using MRI. This detailed anatomical information is crucial for surgical planning, particularly in determining the feasibility of achieving clear margins and thus reducing the risk of local recurrence.
The multiplanar imaging capabilities of MRI allow for the acquisition of images in multiple planes without repositioning the patient, which is invaluable for assessing complex anatomical regions. MRI can provide detailed information on the tumor's circumferential resection margin (CRM), which is a critical factor in surgical decision-making. Understanding the involvement of the CRM helps surgeons plan the extent of resection needed to achieve negative margins, which is associated with improved oncological outcomes.
Despite its advantages, MRI interpretation can be challenging and requires specialized expertise. Variability in MRI image quality and the subjective nature of some interpretative aspects can lead to differences in staging accuracy, particularly in less experienced hands. Furthermore, access to high-quality MRI equipment and trained radiologists may be limited in some healthcare settings, posing a barrier to its widespread use.
c) Integrating F-FDG PET/CT and MRI
The complementary strengths of F-FDG PET/CT and MRI highlight the value of an integrated imaging approach. F-FDG PET/CT's ability to detect distant metastases and MRI's superiority in local staging make them an ideal combination for a comprehensive preoperative assessment of rectal cancer. This integrated approach can enhance staging accuracy, leading to more informed treatment decisions.
By leveraging the metabolic imaging capabilities of F-FDG PET/CT, clinicians can identify patients with distant metastatic disease who may benefit from systemic therapies or palliative care instead of curative surgery. Concurrently, the detailed anatomical information provided by MRI can guide precise surgical planning for those with localized disease, ensuring optimal resection and reducing the risk of local recurrence. The integration of these modalities provides a holistic view of the disease, which is essential for tailoring personalized treatment strategies. Additionally, advancements in imaging technology , such as the development of hybrid PET/MRI systems, could further enhance diagnostic accuracy by combining the strengths of both modalities in a single imaging session. Emerging imaging tracers and techniques may also improve the detection of both local and distant disease, providing more detailed insights into tumor biology.
Therefore, our comparative evaluation of F-FDG PET/CT and MRI for preoperative staging of rectal cancer underscores the necessity of a multimodal imaging approach. Clinicians must carefully consider the benefits and limitations of each modality, alongside patient-specific factors and institutional resources, to select the most appropriate imaging strategy. An integrated approach that leverages the strengths of both F-FDG PET/CT and MRI is essential for achieving comprehensive disease assessment and guiding personalized treatment strategies, ultimately improving patient care and outcomes in rectal cancer.
V. CONCLUSION
In this study we demonstrate that F-FDG PET/CT and MRI are comparable for preoperative staging of rectal cancer, with their own limitations and benefits. MRI provides detailed information about the local tissue involvement, mesorectal fascia and nearby structure involvement and presence of lymph node metastases whereas F-FDG PET/CT is more helpful in detecting distant metastases and tumour metabolism. But as MRI is more readily available and is more cost effective than F-FDG PET/CT in developing countries such as India, it should be used as the imaging modality of choice for pre-operative staging of rectal cancer.



