## I. INTRODUCTION
Breast augmentation is among the most popular elective cosmetic surgeries, reflecting the growing demand for procedures that enhance both form and confidence. Over the past 20 years, innovations in surgical methods have significantly reduced complications and improved patient satisfaction. The breast implant is widely regarded as one of the most pivotal devices in the history of plastic and reconstructive surgery. However, despite half a century of technological advancements, revision rates for breast prostheses remain high, reported at $24\%$ at 4 years and $36\%$ at 10 years [1].
In recent years, the perception of an attractive breast has shifted towards a three-dimensional analyses, with particular attention to shape and preferred proportion patterns [2-5]. Despite this progress, the intermammary cleft (or cleavage) has been insufficiently studied, despite its critical importance in surgical outcomes and patient satisfaction. A major drawback of traditional breast implants is the potential for an unnatural appearance when the balance between soft tissue volume and implant volume is disrupted. Breast implants cannot change the footprint of the breasts, and although they enhance cup size, they do not modify intermammary distance. Many females desire a narrow cleavage distance along with breast augmentation [6,7].
Hybrid breast augmentation offers a solution by combining breast implants with autologous fat grafting to achieve a natural-looking breast contour while reducing the intermammary distance [8]. This technique aims to improve cleavage shape as well as achieve a natural look and feel, which is facilitated by fat grafting. Transferred fat also ensures that the steep curve of the implant take off of the breast mound is modified to a gentle slope, resulting in a more natural shape [9].
The purpose of this study is to evaluate the outcomes of hybrid breast augmentation, particularly its role in remodelling the medial cleavage and reducing the intermammary distance during breast implant surgery. Additionally, the study assesses patient satisfaction with this combined approach.
## II. METHODS
Between January 2021 and September 2024, 131 female patients presented with concerns regarding aesthetically unsatisfactory breasts and sought breast enlargement surgery. A retrospective study was conducted on these patients, all of whom underwent hybrid breast augmentation combining fat injections with silicone breast implants, resulting in 262 treated breasts.
Patients received small- to moderate-volume fat grafts, which were harvested, processed, and implanted using standardized methods. The age range of the patients was 30 to 55 years. Exclusion criteria included an intermammary distance of less than $8\mathrm{cm}$, smoking, and a BMI above $30\mathrm{kg/m^2}$. None of the patients had pre-existing comorbidities. Written informed consent was obtained from all participants before inclusion in the study.
The surgical procedure involved subfascial breast augmentation using silicone implants with a notouch technique. [Fig.1-4] Fat tissue was harvested from the abdominal or thigh area based on patient preference, following tumescent infiltration. Harvesting was performed using a 2.4-mm cannula, and the fat was processed and prepared for grafting.
Fat grafting was performed in the superomedial quadrant of the breast in a fan-like pattern using a 10- mL Luer-Lock syringe attached to a 1.2-mm bulb-tip cannula, until the pre-marked area was visually covered. The volume of fat injected per breast ranged from 50 to $100~\mathrm{mL}$.
All procedures were conducted under general anesthesia. A single dose of 1 g ceftriaxone was administered intravenously as a prophylactic antibiotic one hour before surgery. Patients were ambulated within 4 hours postoperatively and discharged with compression garments over the fat graft harvest areas and sports bras over the breasts.
Data were collected on patient demographics, implant volume, fat graft volume, preoperative and postoperative Breast-Q© scores, pre and 6 months post op measurements of intermammary distance (measurement of between medial most take off point of each breast) and complications. Follow-up evaluations were conducted at 48 hours, 1 week, 3 weeks, 6 weeks, and 6 months, with additional follow-ups scheduled as needed for reported complications. [Fig. 5-8] A statistical analysis was performed comparing preoperative and postoperative Breast-Q© scores. Mean for each part of the questionnaire were collected and compared using a t-test.
Based on Breast-Q® results, patients were classified as follows: "dissatisfied" (total score between 0 and 50), "satisfied" (total score between 51 and 75), and "very satisfied" (total score between 76 and 100).
## III. RESULTS
A total of 131 patients undergoing hybrid breast augmentation were followed up for six months, yielding satisfactory results in terms of achieving a natural feel, enhanced shape, and less visible scarring.
The age of the patients ranged from 30 to over 55 years, with a mean age of $46.5 \pm 5.3$ years. Most patients were in the 41-45 age group (32.1%) and 46-50 age group (31.3%), reflecting a preference for the procedure among individuals in midlife (Table 1).
Postoperative outcomes were favorable, with a mean cleavage distance of $9.5 \pm 1.23$ cm preoperatively, ranging from 8 cm to 13 cm. The postoperative cleavage distance was reduced to $4.74 \pm 0.48$ cm, ranging from 3.4 cm to 5.8 cm, demonstrating consistent and aesthetically pleasing results (Table 2). The change in cleavage distance was statistically significant ( $p < 0.0001$ ).
Implant sizes ranged from 230 cc to 320 cc, with a mean implant size of $271.64 \pm 24.2$ cc (Table 3). Fat grafting volumes varied between 50 cc and 100 cc. The majority of the population $(38.9\%)$ received fat graft volumes in the 50-60 cc range, highlighting the individualized approach of combining implants with fat grafting to achieve optimal outcomes (Table 4).
The procedure demonstrated excellent safety, with no major complications reported in $96.9\%$ of cases. A small percentage of patients $(3.1\%)$ experienced wide scars as the only complication.
Patient satisfaction was high, with $84.0\%$ of patients dissatisfied preoperatively (score 0-50) and $93.9\%$ highly satisfied postoperatively (score 76-100) (Table 5). The mean preoperative satisfaction score was $42.88 \pm 19.3$, while the mean postoperative score was $84.83 \pm 7.6$, statistically highly significant improvement $(p < 0.0001)$.
Table 1: Age Distribution
<table><tr><td>Age (In Years) (n=131)</td><td>Frequency</td><td>Percentage</td></tr><tr><td>30-35</td><td>2</td><td>1.5</td></tr><tr><td>36-40</td><td>14</td><td>10.7</td></tr><tr><td>41-45</td><td>42</td><td>32.1</td></tr><tr><td>46-50</td><td>41</td><td>31.3</td></tr><tr><td>51-55</td><td>26</td><td>19.8</td></tr><tr><td>>55</td><td>6</td><td>4.6</td></tr><tr><td>Mean ± SD</td><td colspan="2">46.5 ± 5.3</td></tr></table>
Table 2: Cleavage Distance
<table><tr><td>Cleavage Distance (cm)</td><td>Pre - Operative</td><td>Post - Operative</td></tr><tr><td>Mean ± SD</td><td>9.5 ± 1.23</td><td>4.74 ± 0.48</td></tr><tr><td>Range</td><td>13 cm - 8 cm</td><td>5.8 cm - 3.4 cm</td></tr><tr><td>Median (IQR)</td><td>9 (1.5)</td><td>4.7 (0.6)</td></tr><tr><td colspan="3">p value < 0.0001</td></tr></table>
Table 3: Implant Size
<table><tr><td>Implant Size (in cc)</td><td>Frequency</td><td>Percentage</td></tr><tr><td>230 - 250</td><td>22</td><td>35.9</td></tr><tr><td>251 - 270</td><td>27</td><td>29.0</td></tr><tr><td>271 - 290</td><td>48</td><td>23.7</td></tr><tr><td>291 - 320</td><td>34</td><td>11.5</td></tr><tr><td>Mean ± SD</td><td colspan="2">271.64 ± 24.2</td></tr></table>
Table 4: Amount of Fat Grafted
<table><tr><td>Fat Grafted Range</td><td>Frequency</td><td>Percentage</td></tr><tr><td>50 - 60</td><td>51</td><td>38.9</td></tr><tr><td>61 - 70</td><td>33</td><td>25.2</td></tr><tr><td>71 - 80</td><td>27</td><td>20.6</td></tr><tr><td>81 - 90</td><td>14</td><td>10.7</td></tr><tr><td>91 - 100</td><td>6</td><td>4.6</td></tr><tr><td>Mean ± SD</td><td colspan="2">63.11 ± 11</td></tr></table>
Table 5: Patient Satisfaction
<table><tr><td>Satisfaction level</td><td>Operative (Frequency)</td><td>Percentage</td><td>Operative (Frequency)</td><td>Percentage</td></tr><tr><td>Dissatisfied (0 - 50)</td><td>110</td><td>4.0</td><td>1</td><td>0.8</td></tr><tr><td>Satisfied (51 - 75)</td><td>21</td><td>6.0</td><td>7</td><td>5.3</td></tr><tr><td>ghly Satisfied (76 - 100)</td><td>0</td><td>0</td><td>123</td><td>3.9</td></tr><tr><td>Mean ± SD</td><td colspan="2">42.88 ± 19.3</td><td colspan="2">84.83 ± 7.6</td></tr><tr><td colspan="5">p value < 0.0001</td></tr></table>
## IV. DISCUSSION
Autologous fat transplantation has long been utilized in facial rejuvenation, but its application in breast surgery has been more limited and controversial. The practice of infiltrating the breast with fat has been debated since its introduction by Neuber over a century ago. Fat grafting to the breast gained renewed interest after the reversal of the 1987 American
Society of Plastic Surgeons' moratorium in 2008 [10]. Over the past two decades, autologous fat injection has gained significant acceptance as a viable soft tissue filler for both small- and large-volume applications. Bircoll (1987) was one of the first to report a case of breast augmentation performed using autologous fat grafts [11].
The primary advantage of composite breast augmentation lies in the ability of the surgeon to customize both the shape and size of the breast by working with two versatile, complementary materials placed in distinct planes. In composite breast augmentation, the core volume projection of the implant is managed, while the natural look and feel of fat are used as an overlay, providing additional volume where necessary. Asymmetries in soft-tissue volume can be addressed by using equal-sized implants and differential fat transplantation to achieve a more natural contour and cleavage [12].
Hybrid breast augmentation is ideal for patients seeking breast implants with the contour and feel of natural breast tissue. The technique combines the advantages of both implants and fat: implants provide core volume projection, while the fat layer enhances the aesthetic outcome, ensuring a natural look and feel [13].
Implants can sometimes appear unnatural without adequate coverage, particularly where they meet the surrounding tissue. The addition of autologous fat helps soften these lines, blending the implant more seamlessly with the surrounding tissue. Fat grafting procedures also assist in correcting breast asymmetries. Women with uneven breast sizes may benefit from this method, as fat can be strategically placed to balance the appearance, enhancing patient satisfaction [14].
The primary goal of hybrid breast augmentation is to enhance breast size and shape. Patients typically seek a more voluptuous look while maintaining natural softness. The combination of implants and fat provides the necessary volume and texture, resulting in a realistic and aesthetically pleasing outcome. This technique is especially appreciated by patients desiring a natural silhouette without sacrificing the firmness and projection offered by implants [15].
In our study, implants were inserted in the subfascial plane. In alignment with Maximiliano et al. [16], autologous fat grafts (AFG) were injected into the superomedial breast quadrant, within the subcutaneous plane, to achieve natural cleavage. The results were satisfactory, achieving balanced volume and shape. A satisfactory aesthetic outcome was attained, with a harmonious breast contour and smooth transition from the upper poles to the implant site.
Advancements in AFG techniques, along with the development of new- generation silicone gel prostheses, have significantly improved the aesthetic results of breast augmentation.[17] Our technique has demonstrated that it is a manageable and predictable procedure, yielding optimal aesthetic results with a harmonious contour, adequate size, and projection. Hybrid breast augmentation, therefore, holds the potential to play a significant role in aesthetic breast surgery, refining the field and providing patients with a natural yet enhanced breast appearance.
## V. CONCLUSION
By ingeniously combining the volumizing power of implants with the natural enhancement of fat grafting, we achieve a harmonious balance between projection and a soft, authentic look.
Fat grafting enhances key aesthetic features—softening the intermammary cleft, creating fullness in the upper and medial poles, and ensuring perfect symmetry between the breasts.
However, to truly understand its full potential, further studies with diverse implant types and a broader patient population are crucial.
### ACKNOWLEDGEMENTS
The authors would like to acknowledge Dr. Adarsh Keshari from APAR health for medical writing assistance and data analysis. (Care Program)
Funding Sources if applicable
None
Ethical Clearance/Statement of Ethics
The study was approved by the Gene Bandhu ethics committee. (Ref- ECG005/2025) The meeting was held on January 17, 2025.
Declaration of conflicts of interest (if applicable)
Authors declare no conflict of interests.


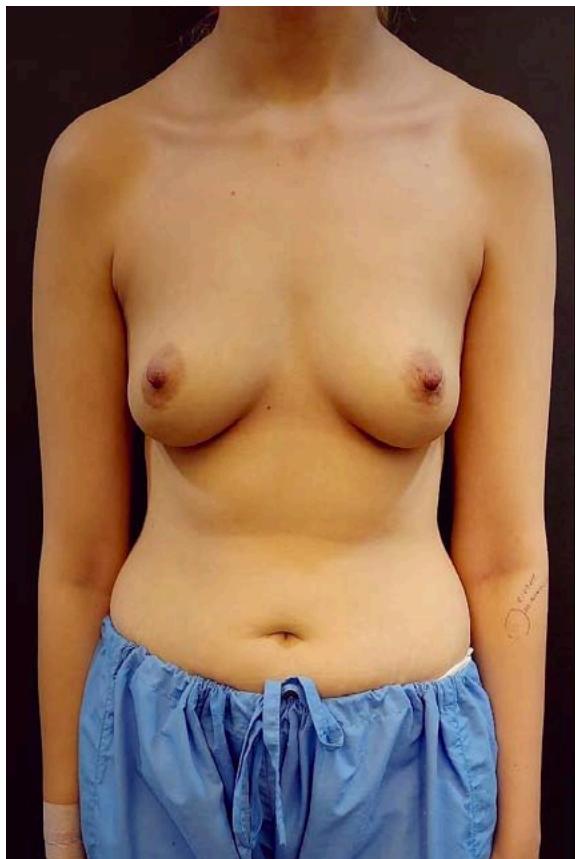 Fig. 6: Before and After of 38 Year Old Tuberous Breast Deformity Correction, 6 Months after 275cc Smooth High Profile Implant in Sub Fascial Plane with 75cc Fat Grafting one Ach Side
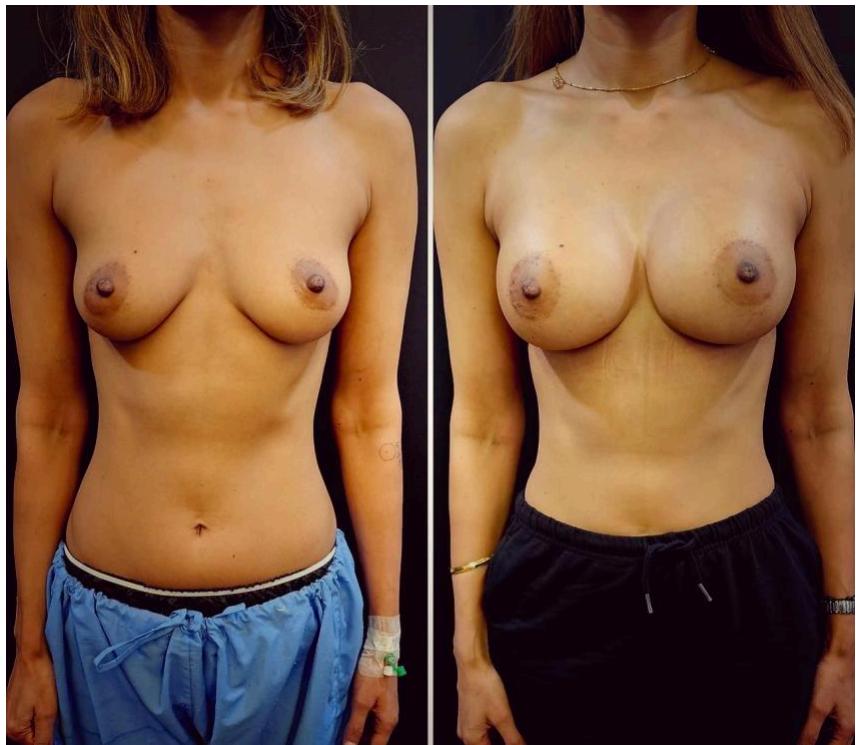
 Fig. 7: Before and After of 34 Year Old, 6 Months after 235 cc Smooth High Profile Implant in Sub Fascial Plane with 45cc Fat Grafting one Ach Side
 Fig. 8: Before and After of 33 Year Old, 6 Months after 305cc Smooth High Profile Implant in Sub Fascial Plane with 40 cc Fat Grafting One Ach Side
Generating HTML Viewer...