The main objective of the present study is to evaluate the therapeutic effectiveness and safety of percutaneous radio-guided chemical ablation with absolute ethanol (96%) in the therapeutic management of cystic and solid lesions. benign localization: thyroid classified EU-TIRADS 2, parathyroid, hepatic, renal, inguino-scrotal, ovarian as well as osteoarticular.
## I. INTRODUCTION
Percutaneous ethanol sclerotherapy is a chemical ablation technique designed primarily for recurrent cystic lesions (1). Alcohol (96%) is the most widely used alcoholic agent, abrading the walls of the liquid lesion and sclerosing the vessels, thus promoting lesion sclerotization. If the liquid is purely colloidal, it is evacuated with a large-gauge needle (14-gauge in our series), then a moderate quantity of alcohol is injected, all of which is withdrawn a few minutes later (2). If the extracted fluid is hematic, the lesion cavity may need to be rinsed one or more times with saline, followed by injection of absolute ethanol, which is then partially reinjected. In cases where the thick partitioned liquid is difficult to evacuate with a large-gauge needle, it can be dissolved by injecting small quantities of absolute ethanol into several areas of the cystic lesion; 2 to 4 days later, the colloidal liquid is fluidized and ready for evacuation or sclerotherapy. In most cases, the procedure is painless. A slight burning pain may be felt when the ethanol is injected and the needle withdrawn, prompting some operators to inject a small amount of $1\%$ lidocaine before withdrawal. This treatment is highly effective, particularly for cysts, with efficacy in excess of $80 - 90\%$. Complications are rare and reversible: thyroid recurrent paralysis, when alcohol leaks out of the thyroid nodule. The patient must be informed of this and, if necessary, asked to sign an informed consent form. This treatment, unjustly ignored in many countries, benefits from a consensual recommendation in the management of cystic thyroid nodules: ETA European Thyroid Association and ATA American Thyroid Association (3) for all thyroid nodules.
## II. MATERIALS AND METHODS
### a) Framework of the Study
The present study was carried out in five hospital institutions in Kinshasa, capital of the Democratic Republic of the Congo; the first of which was at tertiary level; the Cliniques Universitaires de Kinshasa (CUK) and four others at primary level: Center de diagnostic spécialisé et d'imagerie Interventionnelle (CDSII), Hôpital de Kingasani II (HSK II), Clinique la Vie (CV) and Clinique Pistis Médical center (PMC) all in Kinshasa. All these data were collated at CUK, the leading institution of higher education and university in the Democratic Republic of Congo (DRC), located on Mont-Amba, in the Commune of Lemba. They occupy a surface area of 27110 m2 and can be accessed via two routes: Avenue de l'Université and Avenue de la Foire at Rond-Point-Ngaba.
### b) Study Type
This was a descriptive, observational, multicenter study conducted over a six-year period, from April 01, 2018 to April 01, 2024.2. 2 Study participants and design the present work was a descriptive cross-sectional study evaluating the efficacy and safety of percutaneous ethanol sclerotherapy in the treatment of thyroid, hepatorenal, articular and inguino-scrotal cystic lesions through a series of eighty consecutive patients collected in hospital settings in Kinshasa, between April 2018 and April 2024, a period of 6 years. Included in the present study were all patients, regardless of nationality, male or female, of any age, referred for management of a symptomatic cystic lesion in the following locations: thyroid, hepatic, renal, articular, ovarian and inguinoscrotal; carrying images of examinations performed on cliché or on a CD Room with an ultrasound, scan and/or MRI report. All patients were managed according to the pre-established protocol (on D1-J4 and D7). Four ultrasound scanners with linear and convex probes were used. These included two sonoscope light machines, one Phillips U-22 machine and a third Edan machine. These examinations were carried out in triplex Doppler mode. In addition to ultrasound scanners, two CT scanners were used, including a HITACHI 16-bar Eclos model, commissioned in 2011. CT scans were performed on the kidney and liver. These were performed before and after injection of the contrast medium. All examinations were performed in low-dose mode. Patients with solid cystic lesions, symptomatic cystic lesions involving organs not included in the present study, and patients who did not freely adhere to treatment after radiological consultation, were excluded from the study.
### c) Radiological Technique
After skin disinfection of the area of interest with Betadine, we proceeded to puncture-evacuate the cystic contents, using an 18/14 Gauge coaxial depending on the lesion content. Lesion volume and content appearance were strictly studied. When the liquid returned as hematic, the patient received three sessions of sclerotherapy; when the liquid was clear, the patient received one or two sessions of sclerotherapy. Once the entire lesion had been evacuated, $96\%$ ethanol was injected through the co-axial left in place. The amount of ethanol injected was calculated at $15 - 20\%$ of the initial overall volume of the cystic lesion to be treated. The instilled sclerosant was left in place for a few minutes (10 to 20 minutes) before being removed. The liquid was then rinsed and reaspirated, before a small ice bag was placed on the skin for 5 to 10 minutes. At the end of the procedure, a dry, compressive dressing was applied and a short clinical monitoring period of 40 to 60 minutes was used to detect any early complications. Pain after sclerotherapy was assessed at 1st check-up using a visual analogue scale (VAS) ranging from 0 (no pain) to 10 (intense unbearable pain). All patients underwent local anaesthesia and antibiotic prophylaxis. Patients who received all three sessions were treated on day 1, day 4 and day 7. All patients were reviewed at one month, 3 months, 6 months and one year after the first sclerotherapy session. An interview concerning the immediate and delayed after-effects of sclerotherapy was completed at each radiological consultation. The final efficacy of chemical ablation was defined by the absence of cyst reconstitution, the disappearance of pain, and the persistence of a residual quantity of less than $50\%$ of the initial volume at the 1-month follow-up ultrasound. However, in the event of recurrence after two sessions, a third session was systematically performed. In the event of refusal or non-compliance, the patient was referred to the referring physician.
### d) Data Organization and Statistical Analysis
Study data were represented by sociodemographic, clinical, ultrasound and histological variables. Data were organized and encoded in Excel version 2010. R software version 4.1.3 was used for statistical analysis of the study data. Variables were summarized by numbers and proportions, then presented in tables and graphs. A multivariate logistic regression model was used, with the number of drinking sessions of the subject as the dependent variable, using several independent variables (histology, location of the mass, sex of the subject and volume of the mass). For each independent variable, the Odds Ratio and its confidence interval at the 0.05 level of significance were calculated.
## III. RESULTS
Eighty patients were enumerated during the study period, $46.2\%$ male and $53.8\%$ female, giving a sex ratio of $0.83\%$ (Table 1). Patient age ranged from 6 to 75 years, with an average age of $43.5 \pm 17.5$ years (Table 1). The youngest patient was 6 and the oldest 75 (Table 1). The 37-47 age group was the most represented with $26.3\%$ (Table 1). The majority of women were between the ages of 26-36 and 37-47, representing $27.5\%$ of the total workforce (Table 1). A further $17.5\%$ of men were aged between 48 and 58 (Table 1). With regard to the clinical characteristics of the patients, it should be noted that almost $55\%$ of the patients had presented a cervical swelling on physical examination, of whom twenty-four were female and twenty male (Tables 2 and 4). $10\%$ of the patients in our sample had presented a sensation of a mass on the left flank as a clinical complaint. Similarly, $5\%$ of males and $5\%$ of females had presented epigastric tenderness as a clinical complaint (Tables 2, 4). The distribution of patients according to anatomopathological findings showed that $64\%$ of patients referred for sclerotherapy presented an inflammatory smear after cytological analysis of the puncture-drainage fluid (Table 3); $15\%$ of patients in the series presented benign lesions with no signs of atypia, and $2.5\%$ presented a hemorrhagic smear with no atypical cells after cytological assessment. (Table 3). In relation to the distribution of organs treated, $42.5\%$ of lesions treated were thyroid lesions, $32.5\%$ renal lesions, $12.5\%$ liver lesions, $7.5\%$ breast lesions and $5\%$ parotid lesions. (Table 5). The search for factors linked to the number of alcohol sessions carried out per patient revealed that the number of alcohol sessions depended on the type of organ alcoholized, the content of the alcoholized lesion (whether hemorrhagic or purely clear liquid), the patient's sex and, of course, the volume of the alcoholized mass. (Tables: 5, 6, Figure: 1) The relationship between the number of sclerotherapy sessions, the organs treated, the alcohol lesion and the patient's sex, clearly shows that the number of sclerotherapy sessions was increased to two or three for the same patient, when faced with the following situations: a larger lesion volume, a female subject, a hemorrhagic lesion content, or when the lesion treated was intrahepatic (Figure: 1). A comparison of the number of sclerotherapy sessions with the sex and age of patients by organ clearly shows that the number of sessions was very different for the different organs, although not significantly different by sex between patients by organ. However, the age of patients differed according to the organs affected. (Tables: 4, 6).
## IV. DISCUSSION
From April 1, 2018 to April 1, 2024, eighty patients underwent percutaneous sclerotherapy of their lesions using absolute ethanol in hospital settings in Kinshasa. A minimum follow-up period of six months to one year was required to evaluate our results. Sclerotherapy is an ancient technique involving the injection of a cytotoxic solution into a lesion to induce localized necrosis. Absolute ethanol sclerotherapy, or alcoholization, involves injecting highly concentrated ethanol (generally between 90 and $100\%$ ) over a period of a few minutes. Recent advances in minimally invasive techniques have led to the development of alternatives to open or laparoscopic surgery for the treatment of simple, symptomatic cysts in several organs. Simple puncture of these cysts without a sclerosing agent was associated with significant recurrence of up to $80\%$ [4]. Ethanol $99\%$ was more widely used because it leads to rapid destruction of the secretory epithelium (1-3 min), while crossing the fibrous cyst shell very slowly (4-12 hours) and resulting in minimal local or systemic side effects. The most frequent intraoperative complication with this technique remains the risk of bleeding (4-10%). Post-operative infectious complications can reach $10\%$ [5]. None of these complications (hemorrhage or infection) were encountered in our series. We did, however, record one case of hypoglycemic shock, which was rapidly corrected with hypertonic saline at a rate of $1\mathrm{ml}$ per kg of body weight. The latter was probably caused by a prolonged fasting period prior to the procedure. In all cases, the most frequent complication encountered in the present series was the sensation of burning during ethanol injection. In the present series, ethanol was used predominantly $(100\%)$, unlike other sclerosing agents such as Betadine and $75\%$ alcohol, sodium tetradocylsulfate, hydroxypolyethoxydodecane, tetracycline and others. The average volume of ethanol used in the present series was $12.85\mathrm{ml}$; the largest volume of ethanol was $40\mathrm{ml}$ and the smallest volume was estimated at $2\mathrm{ml}$. The average volume of lesions treated was $106.12\mathrm{ml}$, the smallest lesion volume was $4\mathrm{ml}$, and the largest volume was $814\mathrm{ml}$. Several lesion locations were included in the present series, including: thyroid head location with $42.5\%$, renal with $32.5\%$, hepatic with $12.5\%$, mammary with $7.5\%$ and others with $5\%$ (parotid, ovarian, inguino scrotal and osteo articular). This corroborates literature data, insofar as when this technique was first published in Japan by Akamatsu et al. in 1988; several benign cystic lesions treated had been reported among others: thyroidiennes, parathyroid, splenic, hepatic and renal with good efficacy [6-7]. In relation to the frequency of organs treated in the present study, it is established that thyroid nodules were the most treated to the tune of $42.5\%$. It should be noted; that thyroid nodules are common, clinically palpable lesions with a prevalence of $4 - 7\%$ in the general population [1-3]. However, this prevalence increases to $20 - 76\%$ on ultra sonographic examination [1-3]. Percutaneous sclerotherapy has been suggested as an effective alternative, particularly in patients with cystic nodules [1-3]. Simple (purely cystic) cysts, constituting $6 - 28\%$ of all thyroid nodules, are usually benign, filled with cellular debris or blood, and are the result of degeneration or hemorrhage in a hyperplastic nodule. However, data on the results of percutaneous aspiration and ethanol injection (PEI) in resolving thyroid nodules is highly variable in different studies (success rate: $38 - 85\%$ ), which may be due to the different populations studied and the heterogeneous nature of the thyroid nodules evaluated [1-3]. With regard to socio-demographic characteristics, we noted a predominance of women $(53.8\%)$ versus men $(46.3\%)$, giving a sex ratio of $0.83\%$. The 37-47 age group was the most represented, with $26.3\%$. The majority of women were between the ages of 26-36 and 37-47, representing $27.5\%$ of the total workforce. Seventeen-point five percent of men were aged between 48 and 58. From the above, the majority of patients treated in the present study were relatively young women. This may be explained by the fact that the most frequent location of lesions treated was the thyroid. Thyroid nodules are common, clinically palpable lesions, with a prevalence of $4 - 7\%$ in the general population [2,3]. However, this prevalence increases to $20 - 76\%$ on ultra sonographic examination [2,3]. This hypothesis contradicts the appearance of renal cystic lesions, bearing in mind that their incidence increases progressively with age. In Terrada's study, their incidence rose from $5.1\%$ in the fourth decade to $36.1\%$ in the eighth decade, a sevenfold increase [8]. Their prevalence was $22\%$ in a control population over 70 years of age [9]. In relation to the clinical characteristics of the patients, it should be noted that almost $55\%$ of patients had presented with an ante cervical swelling on physical examination, of whom twenty-four were female and twenty male (Tables V and VI). The predominance of ante cervical swelling in the present series, perhaps explained by the fact that the majority of lesions treated were of thyroid [10] location. The distribution of patients according to anatomopathological findings reveals that more than half of the patients in the present series $(64\%)$ had an inflammatory smear on cytological analysis (Table VII); $15\%$ of patients had benign lesions with no signs of atypia, and $2.5\%$ of patients had a haemorrhagic smear with no atypical cells. (Table VII). These data may be justified by a rigorous selection of patients for percutaneous ethanol sclerotherapy. In relation to the distribution of alcoholic lesions by organ, $42.5\%$ of lesions treated were thyroid lesions, while $32.5\%$ of lesions treated were kidney lesions, $12.5\%$ of lesions treated were liver lesions, $7.5\%$ of lesions treated were breast lesions and $5\%$ of lesions treated were parotid lesions. (Table 12). Research into the factors linked to the number of alcohol treatment sessions carried out per patient revealed that the number of alcohol treatment sessions depended on the type of organ treated, the content of the lesion treated (whether thick, haemorrhagic or purely liquid), the sex of the patient and the volume of the cystic mass treated. (Table), 13, Figure 1). Research into the relationship between the number of sclerotherapy sessions, the volume of the lesion to be treated and the patient's sex, shows that the number of sessions during sclerotherapy was increased to two or three sessions for the same patient, when the lesion volume was greater, either when the subject treated was female, or when the lesion content was hemorrhagic, or when the lesion to be treated was located in the liver. (Figure 1); this could be explained by the liver's rich portal and vascular network, likely to cause ethanol to leak out, thus reducing its volume, with a consequent loss of efficacy. A comparison of the number of sclerotherapy sessions with the sex and age of patients by organ shows that the number of sessions was very different for the different organs, with no significant difference in sex between patients by organ. However, the age of patients differed according to the organs affected. (Table 13). According to some studies, including Hanna's, a single injection of ethanol would achieve total cyst regression in only $10-70\%$ of cases [10,14], especially if the cystic volume was large. Repeated injections would significantly improve complete regression $\left\lfloor 11\right\rfloor$ as would catheter drainage for 24 hours $\left\lfloor 12-13-14\right\rfloor$. The combination of the latter two options (puncture drainage followed by a second or third alcoholization) was chosen in our study for large cysts $(>300\mathrm{ml})$; having a greater risk of poor regression or recurrence. In the present series, four of our patients had recurred. There are no studies in the literature evaluating the volume at which a second early instillation of ethanol is worthwhile. The $300\mathrm{ml}$ threshold for defining a large cyst has been set arbitrarily. Many studies use a regression of more than $50\%$ or more than $60\%$ of the cyst from its initial size as a criterion for success. $\left\lfloor 15-16\right\rfloor$. We have chosen as a success criterion a volumetric regression $>50\%$ from the initial size and as a failure a recurrence $>50\%$ from this initial size. Only two patients had incomplete regression, and two others had reconstitution of the cystic mass. Had the volume criterion been used instead of size, their regression would have been classified as successful. In fact, the volume reduction criterion produced much greater differences than the cyst size reduction criterion,
Unfortunately in the present case; we therefore chose to keep the former criterion. The results of this study in terms of volume regression were similar to those observed in the literature, and slightly better in terms of recurrence rate. This could be explained by the systematic nature of a second and/or third alcoholization for cysts at higher risk of recurrence (very large: here, an arbitrary threshold of $300\mathrm{ml}$ was chosen). However, only 4 patients underwent this specific treatment, and a larger number of patients with large cysts would need to be treated in order to confirm these data. The four patients with incomplete regressions had large cystic volumes ( $>600~\mathrm{mL}$ ). However, as we have seen, all patients had resolution of cyst-related symptoms. Although the radiological success rate was $95\%$, the four patients concerned by a therapeutic failure were asymptomatic. The disappearance of cyst-related symptoms also raises the question of whether a second or third operation is justified. Like Hahn [17]. We were able to observe in patients with repeated and early ultrasound controls (controls at 1 month, 3 months, 6 months and one year for some patients) that the decrease in cyst size seems to have continued until the sixth month before stabilizing and with no continuation of regression beyond twelve months. The median follow-up time was 3.97 years, which seemed sufficient to assess efficacy, even if the majority of patients had a follow-up time of less than one year.
## V. CONCLUSION
Radio-guided percutaneous chemical ablation of benign and symptomatic cystic lesions using $96\%$ ethanol should be considered a credible alternative to surgery in the various interventional radiology units in the DRC. It's a simple, minimally invasive technique that can be performed on an outpatient basis under local anaesthetic; it's effective in the medium and long term, inexpensive and enables rapid return to work. It can be recommended even after a recurrence, and does not contraindicate a possible surgical intervention in cases where it is recommended. In the present study, we made the following observations: a predominance of females $(53.8\%)$, with a sex ratio of $0.83\%$, an average age of $43.5 \pm 17.5$ years, predominantly in the 37-47 age bracket, a predominance of antecervical swelling on physical examination in $55\%$ of cases, cytological examination predominated by inflammatory smears and benign lesions with no signs of atypia on anatomopathological examination, thyroid localization of treated lesions predominated in $42.5\%$, an estimated efficacy of $95\%$ (4 cases of recurrence, all of hepatic location) and no major complications following treatment. The ideal dose of ethanol in the present series was calculated on the basis of the initial volume of the lesion treated (10 to $20\%$ of the initial volume).
The good results obtained in the present series are long-lasting, at the cost of rare complications, with a satisfactory cost-effectiveness ratio. The efficacy and safety of these techniques are the result of a rigorous selection of patients to be treated, and the proven expertise of our team. In the present series, ethanol was used in the majority of cases, unlike other sclerosing agents. The average volume of ethanol used was 12.85 ml; the largest volume of ethanol was 40 ml and the smallest volume was estimated at 2 ml. The average volume of lesion treated was 106.12 ml, the smallest volume was 4 ml, and the largest volume was 814 ml. Several lesion locations were included in the present series, including thyroid (42.5%), kidney (32.5%), liver (12.5%), breast (7.5%) and others (5%) (parotid, ovarian, inguino-scrotal and osteoarticular). (Table 12). This corroborates the data in the literature, insofar as when this technique was first published in Japan by Akamatsu et al. in 1988, several benign cystic lesions were reported to have been treated, including thyroid, parathyroid, splenic, hepatic and renal lesions, with good efficacy. Limitations of the present study: The sample size, the average follow-up time, not to mention the fact that the initial volume was calculated using the formula for calculating the volume of a sphere (4/3 R^3), probably overestimating the actual volume. In fact, the radiological diameter measured is the maximum diameter, whereas cysts are rarely perfectly spherical. This may explain the discrepancy between the calculated mean initial volume and the aspirated cystic volume. A three-dimensional CT measurement (in a prospective study) would enable a much more accurate volumetric calculation according to the method of Seoet al. [18]. Protection of human and animal rights: The authors state that this study did not involve subject or animal experimentation.
Study Funding: This study did not receive specific funding from any public or private institution.
Table 1: Patient Distribution by Gender and Age Group
<table><tr><td rowspan="2">Age</td><td colspan="2">Gender</td><td rowspan="2">Total n (%)</td></tr><tr><td>F</td><td>M</td></tr><tr><td>≤ 25</td><td>5</td><td>2</td><td>7 (8,75)</td></tr><tr><td>26-36</td><td>11</td><td>4</td><td>15 (18,75)</td></tr><tr><td>37-47</td><td>11</td><td>10</td><td>21 (26,25)</td></tr><tr><td>48-58</td><td>5</td><td>14</td><td>19 (23,75)</td></tr><tr><td>59-69</td><td>9</td><td>0</td><td>9 (11,25)</td></tr><tr><td>≥ 70</td><td>2</td><td>7</td><td>9 (11,25)</td></tr><tr><td>Total</td><td>43</td><td>37</td><td>80 (100)</td></tr></table>
Table 2: Distribution of Patients According to Clinical, Ultrasound Indications AAD Sex
<table><tr><td></td><td colspan="2">Sex</td><td rowspan="2">Total</td></tr><tr><td>Clinical indications</td><td>F</td><td>M</td></tr><tr><td>History of pancreatitis</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Left flank pain</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Right flank pain</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Epigastric pain</td><td>4</td><td>0</td><td>4(5)</td></tr><tr><td>Left lower back pain</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Left hypochondralgia</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Renitent retro popliteal mass</td><td>1</td><td>1</td><td>2(2,5)</td></tr><tr><td>Left breast mass</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Focus on low back pain</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Sensation of a mass in the left liver</td><td>4</td><td>4</td><td>8(10)</td></tr><tr><td>Sensation of a mass under the right Angulo mandibular</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Epigastric and left flank tenderness</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Cervical swelling</td><td>24</td><td>20</td><td>44(55)</td></tr><tr><td>Right inguinal swelling</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Renitent swelling of the left elbow</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Total</td><td>43</td><td>37</td><td>80(100)</td></tr><tr><td>Ultrasound indications</td><td></td><td></td><td></td></tr><tr><td>Large lobar nodule classified TIRADS 4</td><td>4</td><td>0</td><td>4(5)</td></tr><tr><td>Right retro popliteal cyst</td><td>1</td><td>1</td><td>2(2,5)</td></tr><tr><td>Cystic mass of left liver</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Cystic mass under rightAngulo mandibular</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Solid cystic mass of the left liver</td><td>0</td><td>4</td><td>4(5)</td></tr><tr><td>Left lobar isthmo nodule</td><td>1</td><td>1</td><td>2(2,5)</td></tr><tr><td>Left lobar toto thyroid nodule with degeneration range</td><td>1</td><td>1</td><td>2(2,5)</td></tr><tr><td>No ultrasound information</td><td>30</td><td>30</td><td>60(75)</td></tr><tr><td>Recurrence of a cystic mass of the left liver</td><td>2</td><td>0</td><td>2(2,5)</td></tr><tr><td>Total</td><td>43</td><td>37</td><td>80(100)</td></tr></table>
Table 3: Distribution of Patients According to Pathological Information and Sex
<table><tr><td rowspan="2"></td><td colspan="2">Sex</td><td rowspan="2">Total</td></tr><tr><td>M</td><td>F</td></tr><tr><td>Adenofibroma without signs of atypia</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>benign</td><td>5</td><td>7</td><td>12(15)</td></tr><tr><td>Hemorrhagic smear</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Inflammatory smear</td><td>32</td><td>32</td><td>64(80)</td></tr><tr><td>Total</td><td>37</td><td>43</td><td>80(100)</td></tr></table>
Table 4: Crossed Clinical, Ultrasound and Histological Indications
<table><tr><td rowspan="2"></td><td colspan="4">Histologie</td><td rowspan="2">Total</td></tr><tr><td>Adenofibrome sans signe d'atypie</td><td>Benin</td><td>Frottis hémorragique</td><td>Frottis inflammatoire</td></tr><tr><td>Indications échographiques</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Gros nodule toto lobeire gauche classé TIRADS 4</td><td>0</td><td>2</td><td>2</td><td>0</td><td>4(5)</td></tr><tr><td>Kyste rétro poplite droit</td><td>0</td><td>2</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Masse kystique du foie gauche</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Masse kystique sous angulo mandibulaire droite</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Masse solido kystique du foie gauche</td><td>0</td><td>0</td><td>0</td><td>4</td><td>4(5)</td></tr><tr><td>Nodule isthmo lobeire gauche</td><td>0</td><td>2</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Nodule thyroidien toto lobeire gauche avec plaque de dégénérence</td><td>0</td><td>2</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Pas de renseignements échographique</td><td>2</td><td>4</td><td>0</td><td>54</td><td>60(75)</td></tr><tr><td>Récidive d'une masse kystique du foie gauche</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Total</td><td>2</td><td>12</td><td>2</td><td>64</td><td>80(00)</td></tr><tr><td>Indications cliniques</td><td></td><td></td><td></td><td></td><td></td></tr><tr><td>Antécédents de pancréatite</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Douleur au flanc gauche</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Douleur du flanc droit</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Douleur épigastrique</td><td>0</td><td>0</td><td>0</td><td>4</td><td>4(5)</td></tr><tr><td>Douleurs lombaires gauches</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Hypochondralgia gauche</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Mase rénitrète retro poplite</td><td>0</td><td>2</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Masse du sein gauche</td><td>2</td><td>0</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Mise au point de lombalgie</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Sensation d'une masse du foie gauche</td><td>0</td><td>0</td><td>0</td><td>8</td><td>8(10)</td></tr><tr><td>Sensation d'une masse sous angulo mandibulaire droite</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Sensibilité épigastrique et au flanc gauche</td><td>0</td><td>0</td><td>0</td><td>2</td><td>2(2,5)</td></tr><tr><td>Tumefaction cervicale</td><td>0</td><td>6</td><td>2</td><td>36</td><td>44(55)</td></tr><tr><td>Tumefaction inguinale droite</td><td>0</td><td>2</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Tumefaction rénitrète du coude gauche</td><td>0</td><td>2</td><td>0</td><td>0</td><td>2(2,5)</td></tr><tr><td>Total</td><td>2</td><td>12</td><td>2</td><td>64</td><td>80(100)</td></tr></table>
Table 5: Frequency of Alcohol use by Organ
<table><tr><td>Organs</td><td>Workforce</td><td>Percentage</td></tr><tr><td>Liver</td><td>10</td><td>12,5</td></tr><tr><td>Parothyroid</td><td>4</td><td>5,0</td></tr><tr><td>Kidney</td><td>26</td><td>32,5</td></tr><tr><td>Breast</td><td>6</td><td>7,5</td></tr><tr><td>Thyroid</td><td>34</td><td>42,5</td></tr><tr><td>Total</td><td>80</td><td>100,0</td></tr></table>



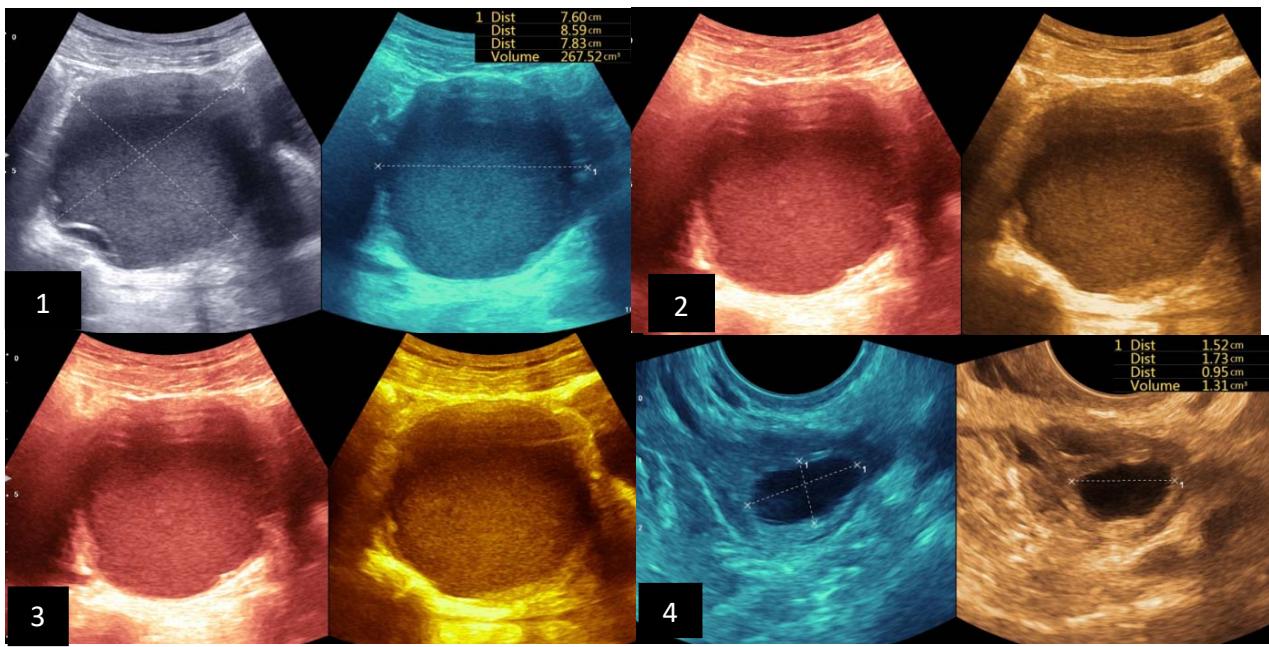
 Iconography A: 1. Ultrasonographic image in B mode, showing a uniloculated cyst, EU-TIRADS 2 of 14.27 ml before sclerotherapy;
2. Ultrasonographic image in B mode after first sclerotherapy session, 3. Ultrasonographic image in B mode, after the second sclerotherapy session, showing complete drying of the cystic nodule, 4. image showing the sero-hematic content of the drained and alcoholic cyst.



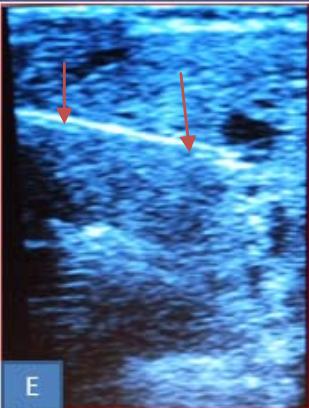
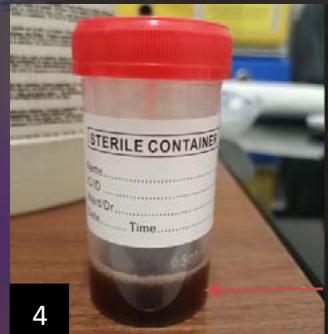
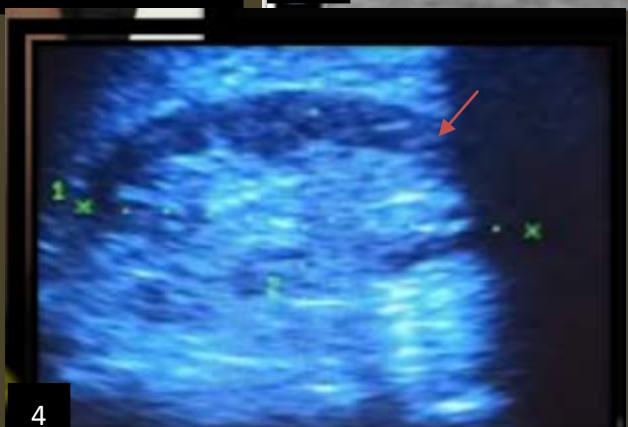
Iconography B: Patient with a 108 ml right isthmo-lobar thyroid hematocele during the first drinking session. A. Materials used before sclerotherapy, B. Image showing a right anterior and lower cervical swelling, Ultra sonographic image: showing a hypoechoic mass dotted around the partitions of 108 ml, D. image showing after ultrasound-guided puncture showing hematic content in the syringe, E. Ultra sonographic image in B mode, showing linear hyper echogenicity of the needle.
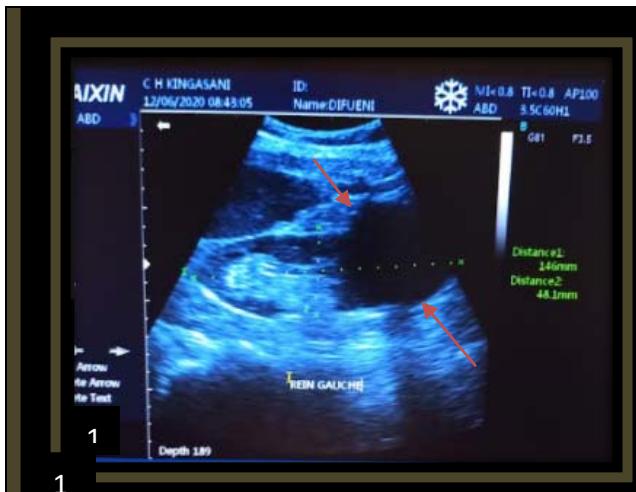
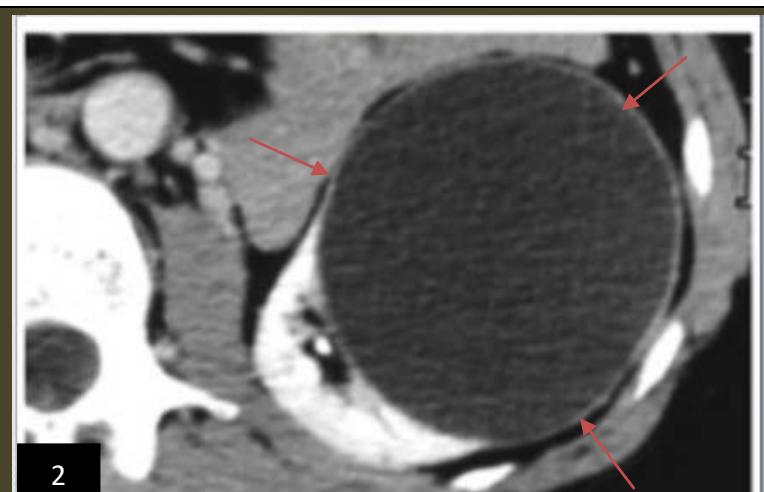




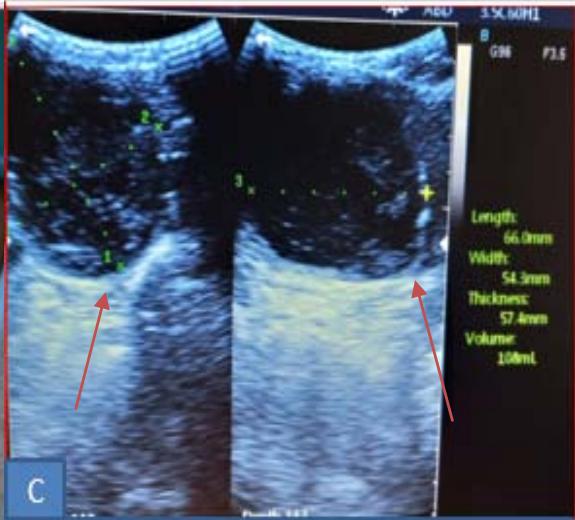
Iconography C: lower left renal polar cystic lesion, alcoholic. Image 1. showing an echo-empty (cystic) left lower renal polar mass,2. CT image showing a left lower polar hypodense mass 3. Ultra sonographic image in B mode showing subcutaneous anesthetic infiltration,4. Image of the left kidney in mode 12 months after sclerotherapy, 5. Image of a clear liquid that had been removed during sclerotherapy.
Generating HTML Viewer...
References
10 Cites in Article
Nicole Iñiguez-Ariza,Robert Lee,Naykky Singh-Ospina,Marius Stan,M Castro (2018). Ethanol Ablation for the Treatment of Cystic and Predominantly Cystic Thyroid Nodules.
Hye Park,Younghee Yim,Jung Baek,Young Choi,Young Shong,Jeong Lee (2019). Ethanol ablation as a treatment strategy for benign cystic thyroid nodules: a comparison of the ethanol retention and aspiration techniques.
Hossein Gharib,Enrico Papini,Jeffrey Garber,Daniel Duick,R Harrell,Laszlo Hegedus,Ralf Paschke,Roberto Valcavi,Paolo Vitti (2016). American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules - 2016 Update Appendix.
R Hanna,M Dahniya (1996). Aspiration and sclerotherapy of symptomatic simple renal cysts: value of two injections of a sclerosing agent..
A Gelet,R Sanseverino,X Martin,J Leveque,J Dubernard (1991). Percutaneous Treatment of Benign Renal Cysts.
N Akamatsu,T Hirai,H Masaoka (1988). Ultrasonically guided puncture of endometrial cysts-aspiration of contents and infusion of ethanol].
Trond Larssen,Asgaut Viste,Arild Horn,Ingfrid Haldorsen,Ansgar Espeland (2016). Single-session alcohol sclerotherapy of symptomatic liver cysts using 10–20 min of ethanol exposure: no recurrence at 2–16 years of follow-up.
Naoki Terada,Kentaro Ichioka,Yosuke Matsuta,Kazutoshi Okubo,Koji Yoshimura,Yoichi Arai (2002). THE NATURAL HISTORY OF SIMPLE RENAL CYSTS.
A Caglioti,C Esposito,G Fuiano,C Buzio,M Postorino,T Rampino,G Conte,A Dal Canton (1993). Prevalence of symptoms in patients with simple renal cysts..
N Akamatsu,T Hirai,H Masaoka (1988). Ultrasonically guided puncture of endometrial cysts-aspiration of contents and infusion of ethanol].
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Tshibasu Tshienda. 2026. \u201cPercutaneous Radio-Guided Chemical Ablation with Absolute Ethanol of Cystic and Solid Lesions in Kinshasa Hospital Environments\u201d. Global Journal of Medical Research - K: Interdisciplinary GJMR-K Volume 25 (GJMR Volume 25 Issue K2): .
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Subject: Global Journal of Medical Research - K: Interdisciplinary
Authors:
Frederick Tshibasu Tshienda, Dr Rémy Kapongo Yobo, Dr Magloire Atantama, Pascal Bayauli Mwasa, Charles Mbendi Lombi, Doudou Batumbo Boloweti, Jean-Marie Kayembe Ntumba, Jean-Marie Mbuyi Muamba (PhD/Dr. count: 0)
The main objective of the present study is to evaluate the therapeutic effectiveness and safety of percutaneous radio-guided chemical ablation with absolute ethanol (96%) in the therapeutic management of cystic and solid lesions. benign localization: thyroid classified EU-TIRADS 2, parathyroid, hepatic, renal, inguino-scrotal, ovarian as well as osteoarticular.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.