
I. INTRODUCTION
Lightning is an aerial electrical discharge, accompanied by a bright light (flash) and a violent detonation (thunder). Lightning is the passage of current through the human body or an animal. In general, a complete lightning strike lasts from 0.2 to 2 seconds.
We describe in this case report the The electrical parameters of the discharge are the intensity which can reach values higher than 200 000 amperes. The voltage seems to be in the range of 10 to 100 million volts. The temperature can reach . [1]
A lightning strike can result in significant damage to the human body through three main mechanisms: cardiac arrest, inhibition of respiratory centers and brain damage.
We describe in this case report the circumstances of a lightning strike of a patient on the landing field of the airport of Bunia who sheltered under an airplane whose major clinical manifestation was a generalized seizure and we discuss the modalities of management and prevention of such a particular accident.
a) Clinical case
We received on Sunday the 22t of January 2023 around 12H40 p.m., at MONUSCO Level 2 Hopsital of
Bunia, Democratic Republic of Congo, Mr M.P a 38-year-old man with no medical history for a sudden loss of consciousness and seizures after a thunder lightning strike at 11 a.m. when working in maintenance of a plane at Bunia airport.
When it was raining heavily, the patient took shelter under the wing of the plane where a lightning strike occurred. The electric shock was transferred to the patient and he suddenly fell to the ground and presented a generalized seizure with loss of urine, which stopped spontaneously after thirty seconds.
The patient was immediately transferred to our hospital by the fire fighters team present at the scene.
Initial clinical assessment found an unconscious patient with a GCS of 9/15. Pupils were equal and reactive. There were no ongoing clinical seizures and there was no evidence of head trauma on clinical examination.
He otherwise presented with stertorous breathing, with desaturation at on room air and polypnea at 35 cycles per minute, auscultation finds rightRonchi with signs of pulmonary aspiration.
He was hemodynamically stable with blood pressure at , and tachycardia at . The pulses were present and symmetrical, and cardiac auscultation was normal.
The abdomen was soft, there was no external burning and the rest of the clinical examination was without abnormalities, the temperature was and the capillary blood glucose was .
After conditioning and monitoring, the patient was placed in a half-seated position with oxygen therapy through a high concentration mask at 10 liters per minute and a peripheral venous line was taken with of isotonic saline.
The patient became agitated which led us to administer of Midazolam IV and analgesia with of Paracetamol in slow infusion.
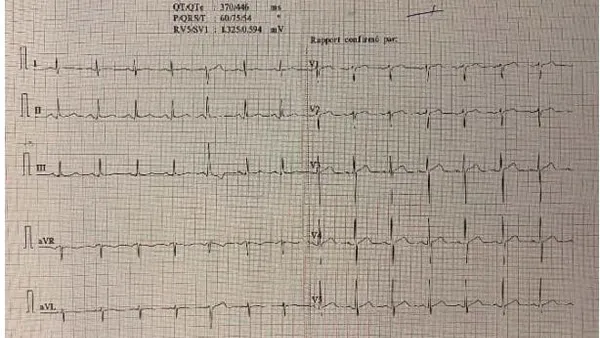
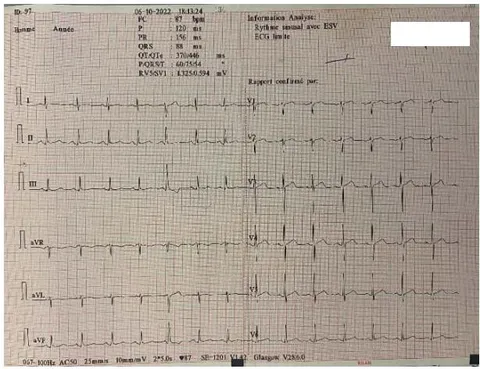
The EKG was without abnormalities, with a regular sinus rhythm at 87 bpm without repolarization or conduction disorders. (Figure 1)
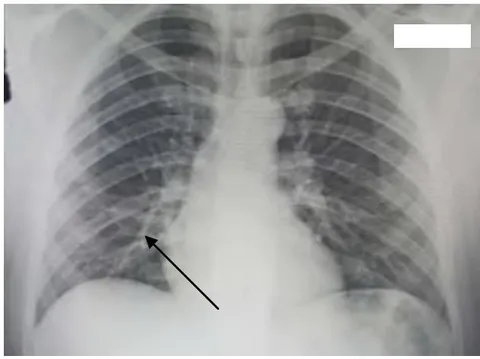
Chest X-ray showed a small basal alveolar image on the right, consistent with gastric aspiration. (Figure 2)
An abdominopelvic ultrasound in search of a peritoneal effusion or a lesion of a solid organ was without abnormalities.
The patient became increasingly calm and cooperative with total amnesia of the circumstances of the accident.
Blood exams showed hemoglobin at , hematocrit at , white blood cells at and platelets at .
The blood ionogram showed a Natremia of 133 mmol/l, a Kalemia of 3.7 mmol/l, a Chloremia of 111 mmol/l, a Bicarbonate of 24 mmol/l and a Phosphorus of 5.5 mg/l.
Blood glucose was , urea and creatinine .
The hepatic enzymes was normal with ASTat 61 IU/l, ALT at 30 IU/l, total Bilirubin at 14 mg/l, PAL at 70 IU/l, GGT at 67 IU/l and Albumin at 32g/l.
Muscle enzymes and lipasemia were normal.
Troponin was normal at
A computerized tomography scan of the head was obtained and was normal, including normal gray-white differentiation, no hemorrhage, or mass effect.
He had pain and paresthesias in both lower limbs, which is why he was put under paracetamol analgesia and under amoxicillin clavulanic acid for aspiration.
After few hours, he was fully conscious and was able to eat and drink. The patient was discharged from the hospital on the third day. He was able to ambulate and had a normal neurological examination and normal mental status. He was awake and able to follow commands.
The patient was referred to a higher level hospital in the capital Kinshasa for further examination and psychological assessment.
II. DISCUSSION
Lightning strikes are a serious accident with a high morbidity and mortality rate. If one out of three
lightning victims dies, seven out of ten survivors have permanent repercussions that are often disabling. However, evidence of lightning injuries is restricted to case reports and nonsystematic reviews. [1]
A distinction must be made between the direct and indirect effects of lightning strikes. Direct effects are due to the release of thermal, light and sound energy but differ according to the type of lightning strike. [2] When the current crosses the heart, it can cause cardiac arrest by asystole or ventricular fibrillation, myocardial ischemia or rhythm disorders. The danger depends on the intensity of the current, its duration and the time of passage in relation to the cardiac cycle.
When the current crosses nerve structures, it can cause consciousness and neurovegetative disorders.
This can lead to deep coma and immediate or delayed respiratory arrest, from minutes to hours. [3]
The frequency of cephalic burns attests to the frequency of cephalic passage of the current.
The neurological manifestations of a lightning strike are extremely varied. They can be serious cerebral lesions such as cerebral haemorrhages with extradural, subdural or intracranial haematoma, secondary to projections and to the effects of the "blast" on the brain, or temporary symptomssuch as loss of consciousness, anterograde amnesia or also anxiety, agitation, irritability, apathy, headaches, cranial nerve damage, paresis or transient paralysis. These symptoms disappear within hours or months. [4]
The respiratory distress is due to the sideration of the respiratory centers by the passage of the current.
The passage of current can also cause electrothermal burns. The muscular masses and the vascular-nervous axes are particularly exposed. The electrical resistance of the latter being low, the intensity delivered locally is high.
For indirect effects, thermal and mechanical energy is released near the lightning channel producing the same effects as an explosion: burns and/or barotrauma.
It is also necessary to point out the posttraumatic stress disorder, sometimes very disabling.
From an electrical point of view, when the discharge crosses the body and the intensity reaches a peak of about 1,000 amps, the potential difference between the head and the feet reaches 300,000 volts. The total duration of a lightning strike is on average 10 to 20 milliseconds. The bypass arc and the brevity of the electrification have a life-saving effect. [5] In our case, the major clinical manifestation was seizures followed by a post-critical coma after transfer of the electric current through the cephalic extremity of the patient who sheltered directly below the aircraft's wing.
All airplanes are equipped with lightning protection devices that discharge any electrical build-up conducting the current through the metal hull to the outside which transmitted it to the patient in our case. [6]
The management of these victims is not specific but all aspects of management must be considered. Consequently, the initial clinical assessment must be exhaustive, and the management complete.
The lightning victim is often electrically shocked, burned, injured, possibly polyfractured or even polytraumatized, sometimes hypothermic and psychologically shocked. [7]
The treatment of each injury is essentially symptomatic. The management of a cardiac arrest is not specific. Cardiopulmonary resuscitation is usually prolonged, especially if it could be initiated early, because of the good prognosis of cardiac arrest in these circumstances and the frequent hypothermia. [8] In our patient, the management consisted of treatment of the seizure and management of respiratory distress and recovery was rapid and complete.
Prevention remains the most effective way to fight against these serious accidents, especially in tropical regions particularly exposed to a high frequency of thunderstorms. The most effective means of this prevention is to take refuge as soon as possible in a raise awareness of the potential dangers of lightning. [9]
III. CONCLUSION
Lightning strikes have high morbidity and mortality rates. However, evidence of lightning injuries is restricted to case reports and series and nonsystematic reviews.
Most damage from lightning injuries is cardiovascular and neurological, although an individual can experience complications with any of their vital functions.
It is vital that every lightning strike patient is treated according to standard trauma guide- lines, with a specific focus on the possible sequel of lighting injuries.
All health-care professionals should acknowledge the risks and particularities of the lighting strike injuries to optimize the care and outcomes of these patients.
Declarations of Competing Interest
None.
Source of funding
No funding was received.