Systemic Arterial Hypertension (SAH) is the most important risk factor for the development of cardiovascular diseases being one of the most prevalent diseases worldwide. Tobacco use has been linked with the development of systemic arterial hypertension or with a difficult control of it, However, it has not yet been universally accepted or demonstrated whether this relationship is directly proportional to vascular damage in people who consume it. The purpose of the study is to compare the effect of smoking on hypertensive smokers vs nonsmoking hypertensive patients.
## I. INTRODUCTION
Systemic Arterial Hypertension (SAH) is the most common risk factor for the development of cardiovascular diseases, it is diagnosed when blood pressure (BP) is $\geq 140 / 90 \mathrm{mmHg}$ after repeated examination. HAS has been divided into primary and secondary HAS, with primary (essential) multifactorial HAS, with direct effects on cardiovascular and renal structure and function, while secondary HAS occurred as a consequence of one or several diseases, half of hypertensive people do not have adequate BP control and of these, only half are controlled. Worldwide, the prevalence of resistant hypertension is $10.3\%$ (Guirguis-Blake et al. 2021). The main risk factors for developing HAS are advanced age (Campos-Nonato et al. 2021), sex, obesity, family history of HAS (being 2 times more common in subjects who have 1 or 2 hypertensive parents), black population, reduced number of nephrons, low socioeconomic level, high intake of sodium $>3$ g/day, excessive alcohol intake, physical inactivity, diabetes mellitus, family history of premature brain vascular disease in 1st degree family, it has also been found that exposure to tobacco is related to a difficult control of blood pressure levels requiring treatment with 2 or more antihypertensive drugs (Guirguis-Blake et al. 2021). According to a study by Kaplan et.al., smoking $>5$ packs of cigarettes per year increases the risk of hypertension up to $30\%$ not being proportional the percentage of cigarettes with a higher risk of suffering hypertension or a difficult hypertension control (Kaplan et al. 2021). In addition, smoking has been directly linked to ischemic strokes in young adults, this is directly proportional to the number of cigarettes smoked during their lifetime (Markidan et al. 2018), the effects of electronic cigarettes are currently under investigation, however, more research is needed(Shi et al. 2023). It has also been related that the increased risk of hypertension could be attributed to low levels of vitamin D induced by exposure to tobacco, this has been demonstrated by measuring cotinine in the body, which is a chemical substance formed by the breakdown of nicotine in the body, used to measure active and passive smoking, having vitamin D deficiency increases the concentration of cotinine in the body, which increases the risk of hypertension (Wu et al. 2022).
Several studies have evaluated the acute effect of cigarette smoke on blood pressure (BP) and have shown consistent results that cigarette smoking temporarily increases BP. This could be explained by the effect of nicotine on the activation of the sympathetic nervous system; however, chronic smoking should not be overlooked as this behavior leads to several harmful effects on the cardiovascular system (Chen et al. 2022a).
Environmental factors, air pollution and green spaces have been associated with hypertension in the field of environmental epidemiology (Chen et al. 2022b).
The increase in arterial stiffness occurs with old age, with the development of chronic conditions such as high blood pressure and the presence of cardiovascular risk factors such as smoking, it has been shown that these two factors make a marked increase in arterial stiffness (Scallan et al. 2010). Levenson et.al. decided to analyze the different independent cumulative effects of hypertension and smoking, they shown that hypertension and smoking affect blood flow properties and arterial wall behavior, these changes are characterized by several abnormalities such as increased blood and plasma viscosity, increased hematocrit, and blood proteins (Levenson et al. 1987).
Smoking undoubtedly confers a significant cardiovascular risk and therefore smoking cessation is one of the best cost-effective measures in the field of medicine. Certain observations have documented that smokers who remove smoking before middle age typically have a life expectancy like non-smoking population (Lu et al. 2018). According to research by Tamotsu Nagao et. al. concluded that by reducing alcohol intake and smoking, the risk of hypertension is considerably reduced (Nagao et al. 2021). As mentioned above, chronic smoking has a direct influence on the development of vascular resistance, producing systemic arterial hypertension regardless of age, sex, and environmental factors, that's why it is of great relevance to know how the increase of blood pressure develops in smoker patients. Smoking has been linked to the use of 2 or more medications for the proper control of arterial hypertension (Kaplan et al. 2021), which leads us to a public health problem and health expenses.
## II. METHODS
Our study is an observational, cross-sectional, prospective, projective, descriptive, and comparative study, the research was carried out in the General Hospital of Zone Number 58 and in the General Hospital "La Villa" Mexico. We interviewed 409 patients aged 40 to 60 years with a diagnosis of SAH through a google forms questionnaire. These patients were divided into two groups depending on smoking history. Pregnant patients, patients with comorbidities, such as chronic kidney disease, pheochromocytoma, vascular or renal anatomical abnormalities were not included, and incomplete questionnaires were removed. The protocol was reviewed and approved by the Research Ethics Committee and the Local Health Research Committee of the Mexican Social Security Institute.
Data analysis was performed using the SPSS and STATA v.14.2 program. The normality test of the variables was calculated using the form measures of bias and curtosis, as well as the Shapiro-Wilks test. The frequency measure to estimate smoking prevalence was obtained by the ratio of people who currently smoke divided by the total sample, multiplied by 100 for its interpretation in percentages. The statistical significance value was established at $p < 0.05$, with a $95\%$ Confidence Interval(Cl).
## III. RESULTS
### 1. Characterization of the study population according to sex
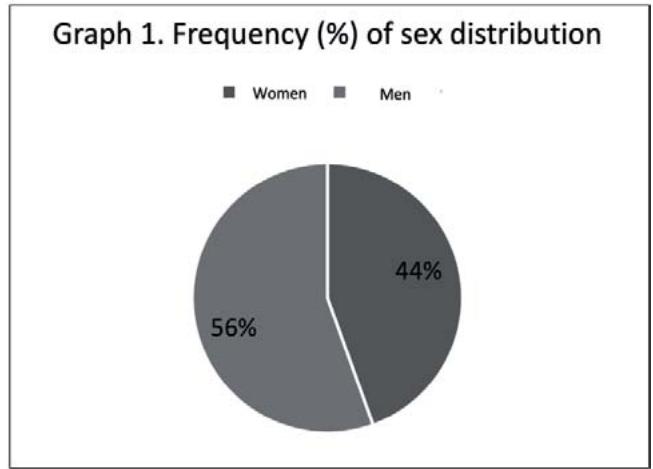
Of a total of 409 patients, $55.5\%$ were men and $44.5\%$ were women, $63.7\%$ were aged between 55 and 60 years and the most frequent school level was primary school $(42.8\%)$, followed by high school $(45.8\%)$, and University $(20.3\%)$ (Table 1) (Graph 1).
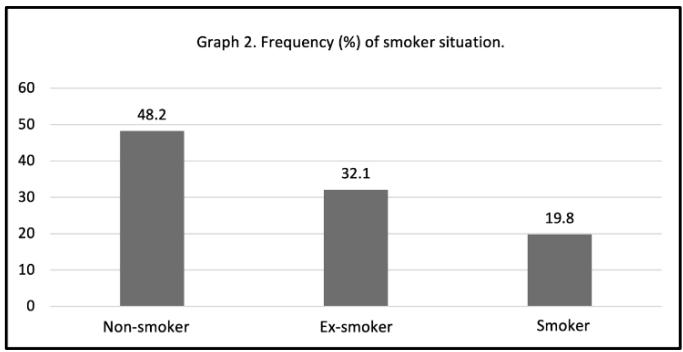
Of the 409 patients, $48.2\%$ have never smoked, $32.1\%$ are former smokers and $19.8\%$ are active smokers (Graph 2).
Almost half of the patients $(44.6\%)$ used one antihypertensive drug to control their BP, followed by those who used two $(37.8\%)$, three $(15\%)$ and four drugs $(2.5\%)$.
Table 1: Study population characterization (n=409).
<table><tr><td>Variables.</td><td>Total (n=409) (%)</td></tr><tr><td>Sex</td><td></td></tr><tr><td>Women</td><td>182 (44.5)</td></tr><tr><td>Men</td><td>227 (55.5)</td></tr><tr><td>Age (n=408)</td><td></td></tr><tr><td>40 to 50 years old</td><td>69 (16.9)</td></tr><tr><td>50 to 55 years old</td><td>79 (19.4)</td></tr><tr><td>55 to 60 years old</td><td>260 (63.7)</td></tr><tr><td>Schooling (n=408)</td><td></td></tr><tr><td>I don't write and read</td><td>8 (2.0)</td></tr><tr><td>I only know how to write and read</td><td>13 (3.2)</td></tr><tr><td>Primary school</td><td>101 (24.8)</td></tr><tr><td>High school 1</td><td>91 (22.3)</td></tr><tr><td>High School 2</td><td>96 (23.5)</td></tr><tr><td>University</td><td>83 (20.3)</td></tr><tr><td>Master's degree</td><td>13 (3.2)</td></tr><tr><td>PhD</td><td>3 (0.7)</td></tr><tr><td>Smoking (n=405)</td><td></td></tr><tr><td>Never</td><td>195 (48.2)</td></tr><tr><td>Ex smoker</td><td>130 (32.1)</td></tr><tr><td>Smoker</td><td>80 (19.8)</td></tr><tr><td>SAH evolution (years) (n=401)</td><td></td></tr><tr><td><10 years</td><td>197 (49.1)</td></tr><tr><td>10-20 years</td><td>122 (30.4)</td></tr><tr><td>20-30 years</td><td>50 (12.5)</td></tr><tr><td>>30 years</td><td>32 (8.0)</td></tr><tr><td>Number of antihypertensive drugs (n=399)</td><td></td></tr><tr><td>1</td><td>178 (44.6)</td></tr><tr><td>2</td><td>151 (37.8)</td></tr><tr><td>3</td><td>60 (15.0)</td></tr><tr><td>4</td><td>10 (2.5)</td></tr></table>
#### 2. Characterization of the study population according to smoking history
Among former smokers, $59.2\%$ were men, a similar proportion in those current smokers $(61.2\%)$, being more frequent to find women without a history of smoking $(71.8\%)$ (Table 2).
In the three categories according to smoking history, more than half of the population was aged between 55 and 60 years. Regarding schooling, among non-smokers it was more common to find people with the primary school level (28.7%) followed by high school (21.5%). In former smokers and smokers, the highest proportion was found in those with high school education (25.4% and 31.3%, respectively).
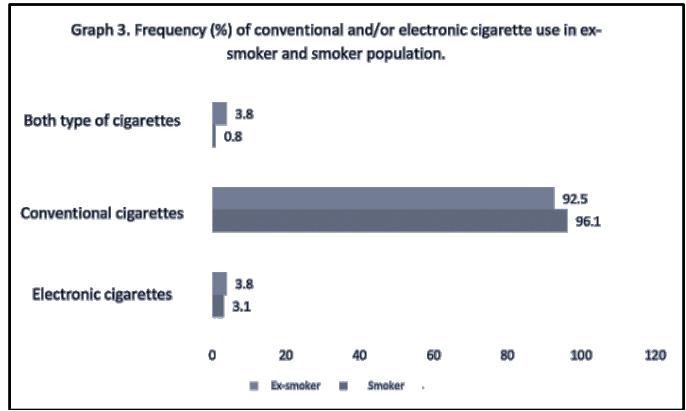
The type of cigarette most used among smokers and ex-smokers was conventional cigarette (96.1% and 92.5%, respectively), only $3\%$ used electronic cigarettes and among ex-smokers, $0.8\%$ employed both, and in the case of smokers it was $3.8\%$ (p value $< 0.000$ )(Graph 3).
The World Health Organization (WHO) classifies smoking severity according to cigarettes consumed per day, mild (less than 5 cigarettes per day), moderate (6 to 15 cigarettes per day) and severe (more than 16 cigarettes per day)(Londoño Pérez et al. 2011; Chang et al. 2021). In our study, most smokers were classified as
mild smokers (62.8% and 58.2%), followed by moderate smokers (27.7% and 35.4%), and 15.5% of former smokers were classified as severe smokers, compared to 6.3% of smokers.
A higher prevalence of cases with less than 10 years of diagnosis of SAH was observed in the categories of former smokers (50%), smokers (53.2%) and non-smokers (47.9%), while the minority of patients had a diagnosis over 30 years of evolution.
Finally, with respect to the number of antihypertensives used to treat SAH, a similar proportion was found among the categories of former smokers, smokers, and non-smokers, being more than $40\%$ those who use a single antihypertensive, followed by two antihypertensives (greater than $30\%$ ), three antihypertensives (greater than $10\%$ ), and finally, less than $4\%$ employed four or more antihypertensives (Graph 4).
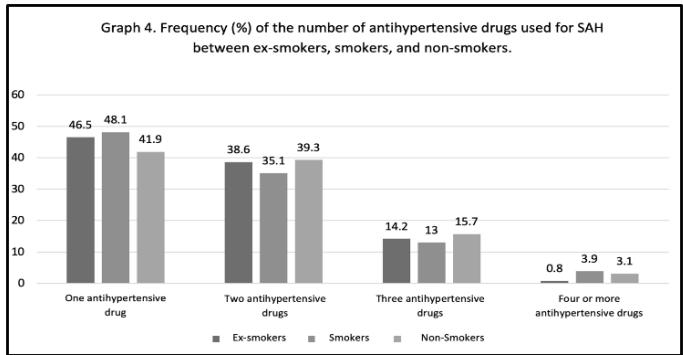
Table 2: Population characterization according to smoking history.
<table><tr><td>Variables</td><td>Ex-smoker (n=130)</td><td>Smoker (n=80)</td><td>No smoker (n=195)</td><td>P Value (95% CI)</td></tr><tr><td>Sex</td><td></td><td></td><td></td><td rowspan="3">0.000</td></tr><tr><td>Women</td><td>53 (40.8)</td><td>31 (38.8)</td><td>140 (71.8)</td></tr><tr><td>Men</td><td>77 (59.2)</td><td>49 (61.2)</td><td>55 (28.2)</td></tr><tr><td>Age (n=408)</td><td></td><td></td><td></td><td></td></tr><tr><td>40 to 50 years old</td><td>15 (11.6)</td><td>21 (26.3)</td><td>33 (16.9)</td><td rowspan="3">0.072</td></tr><tr><td>50 to 55 years old</td><td>27 (20.9)</td><td>17 (21.3)</td><td>35 (18.0)</td></tr><tr><td>55 to 60 years old</td><td>87 (67.4)</td><td>42 (52.5)</td><td>127 (65.1)</td></tr><tr><td>Schooling (n=408)</td><td></td><td></td><td></td><td></td></tr><tr><td>I don't write and read</td><td>2 (1.5)</td><td>-</td><td>6 (3.1)</td><td rowspan="8">0.416</td></tr><tr><td>I only know how to write and read</td><td>2 (1.5)</td><td>2 (2.5)</td><td>8 (4.1)</td></tr><tr><td>Primary school</td><td>30 (23.1)</td><td>14 (17.5)</td><td>56 (28.7)</td></tr><tr><td>High school 1</td><td>31 (23.9)</td><td>17 (21.3)</td><td>42 (21.5)</td></tr><tr><td>High School 2</td><td>33 (25.4)</td><td>25 (31.3)</td><td>38 (19.5)</td></tr><tr><td>University</td><td>29 (22.3)</td><td>17 (21.3)</td><td>37 (19.0)</td></tr><tr><td>Master degree</td><td>2 (1.5)</td><td>4 (5.0)</td><td>7 (3.6)</td></tr><tr><td>PhD</td><td>1 (0.8)</td><td>1 (1.3)</td><td>1 (0.5)</td></tr><tr><td>Type of cigarette</td><td></td><td></td><td></td><td></td></tr><tr><td>Conventional</td><td>124 (96.1)</td><td>74 (92.5)</td><td>-</td><td rowspan="3">0.000</td></tr><tr><td>Electronic</td><td>4 (3.1)</td><td>3 (3.8)</td><td>-</td></tr><tr><td>Both</td><td>1 (0.8)</td><td>3 (3.8)</td><td>-</td></tr><tr><td>Smoker severity (n=208)</td><td></td><td></td><td></td><td></td></tr><tr><td>Mild</td><td>81 (62.8)</td><td>46 (58.2)</td><td>-</td><td>0.03</td></tr><tr><td>Moderate</td><td>28 (27.7)</td><td>28 (35.4)</td><td>-</td><td></td></tr><tr><td>Severe</td><td>20 (15.5)</td><td>5 (6.3)</td><td>-</td><td></td></tr><tr><td>Smoking Index</td><td></td><td></td><td></td><td></td></tr><tr><td>Mild risk (<10)</td><td>96 (73.9)</td><td>62 (77.5)</td><td>-</td><td>0.422</td></tr></table>
#### 3. Relationship between the diagnosis of arterial hypertension and smoking history
Through the Pearson correlation, a weak negative relationship of-0.10 was observed between the years of diagnosis of arterial hypertension and the smoking index a lower year of diagnosis of arterial hypertension, lower the smoking index $(p = 0.8850)$.
In addition, a positive relationship of 0.3672 was observed between the years of diagnosis of SAH and the number of antihypertensives used, that is, to older years of diagnosis of arterial hypertension, greater need to employ more antihypertensive (p value $< 0.000$ ).
## IV. DISCUSSION
In our research we observed that mostsmoker patients are men, for that reason we can associate it with sex since the majority of patients with lung diseases or even with Chronic Obstructive Pulmonary Disease (COPD) are mostly men, so also that men smoke more than women has a socio-background cultural since the Latin American idiosyncrasy urges the male to a greater consumption of substances(Kuntz et al. 2018; Chang et al. 2021), also the majority of our population is between 55 to 60 years of age $(63.7\%)$, which gives us to understand that the older group smoked or smoked more than the younger people $(16.9\%$ are 40 to 45 years old and $19.4\%$ are 50 to 55 years old)(Agustí and Hogg 2019).
Subsequently, if we analyze the time taken by each patient with the diagnosis of SAH, most of patients have less than 10 years of evolution (about $49.1\%$ ) and only $8\%$ had more than 30 years of evolution, therefore we observe that in several cases of our population group the onset of SAH occurs in people who are adults or elderly and this is not directly related to smoking but to the aging process. Although active smoking poses a significant cardiovascular risk, the effect of passive smoking on hypertension is rarely studied. According to
Zhang et. al. passive smoking is significantly associated with an increased prevalence of hypertension, as well as a lower rate of disease control(Zhang et al. 2021).In our study passive smoking was not valued and the final results did not coincide with the results of Zhang, we considered that race and ethnicity were decisive for the results obtained.
Furthermore, it was observed that about half of the patients was treated with a single antihypertensive drug (about $44.6\%$ ), while only $37.8\%$ use two, $15\%$ employed three, and $2.5\%$ used four antihypertensives drugs, for this reason we perceive that most patients having little time being hypertensive require fewer doses of drugs to achieve their antihypertensive treatment goals, however, there is also a minority that requires four or more drugs, we linked this relationship with a greater number of years of SAH evolution, which coincides with the recent literature. Regarding the patient's schooling, we found a significant relationship with smoking, since a large number of our patients reported smoking during teenage, specifically during high school, at $25.4\%$ and $31.3\%$ respectively, whereas non-smoking patients were people with $28.7\%$ of primary school attendance, which reflects that during the process of teenage and the search for identity is yielded to social pressure for the use of harmful substances, among them tobacco, so smoking as psychosocial factors play an important role in the development of hypertension (Wu et al. 2016; Herrera et al. 2017).
In our population the use of electronic cigarettes was studied, however, the relationship with hypertension was not statistically significant, we consider that the variable and the size of the population consuming electronic cigarettes was not sufficient. The relationship between these two variables is currently being studied (Ruokolainen et al. 2021; Falk et al. 2022). According to the WHO classification we can observed that the correlation of tobacco in patients with SAH does not reflect a significant statistical relevance since our patients are mostly mild smokers and therefore due to the inequality in the number of participants corresponding to each degree of smoking index would need to perform more studies to obtain evidence focused on moderate and severe smoking groups. Currently there are no studies that relate the smoking index with SAH, so it cannot be assert that such a relationship exists, and in turn we believe that more research is needed (Zhao et al. 2023). After reviewing the data we can associate the years suffering from hypertension and consumption of antihypertensive drugs since the greater number of years SAH evolution, the greater amount of consumption of antihypertensives drugs, in the matter of SAH and smokers we can say that with less years being hypertensive decreases the value of smoking index of our population, which shows us that if there is influence of tobacco consumption in the hypertensive population.
## V. CONCLUSIONS
For years the relationship between hypertension and tobacco consumption has been the subject of discussion among the scientific community. In multiple scientific articles it has been described that there is no relevant relationship between these two factors while in other publications it is mentioned that if a relationship exists, the relationship between smoking and patients who have been diagnosed with high BP for years opens up a series of interesting proposals to carry out more in-depth and detailed research in the Latino American population, we conclude that patients who have been smoking for more than 30 years tend to have a higher smoking index and therefore consume more antihypertensive drugs so, the more tobacco consumption and longer being hypertensive, greater are the pulmonary complications. In addition, the patients who have stopped smoking or never smoked have a better control of BP, since we found that, to the lesser year of diagnosis of SAH, fewer antihypertensive drugs used in BP control.
### List of Abbreviations:
- Systemic Arterial Hypertension (SAH)
- Blood Pressure (BP)
- World Health Organization (WHO)
- Chronic Obstructive Pulmonary Disease (COPD)
- Confidence Interval (CI)
Declaration Statements
Ethical Approval: The protocol was reviewed and approved by the Research Ethics Committee and the Local Health Research Committee of the Mexican Institute of Social Security; this study did not involve animals.
Consent for Publication: No personal data, images or videos were collected from patients.
Availability of Data and Materials: Data collection was conducted with a questionnaire conducted at Google Forms, while data analysis was performed using the SPSS and STATA v.14.2 program.
Conflict of Interest: The authors declare that they have no conflict of interest.
Financing: None
Authors' Contributions: SP performed data collection, first version of the manuscript, graphs and tables, GL performed statistical analysis, JM collaborated with the final version of the manuscript and manuscript translation, JR participated in data collection, all authors read and approved the final manuscript, RB was dedicated to coordinating the research project.
Generating HTML Viewer...
References
22 Cites in Article
A Agustí,J Hogg (2019). Update on the Pathogenesis of Chronic Obstructive Pulmonary Disease.
Ismael Campos-Nonato,Lucía Hernández-Barrera,Cecilia Oviedo-Solís,Dolores Ramírez-Villalobos,Bernardo Hernández-Prado,Simón Barquera (2021). Epidemiología de la hipertensión arterial en adultos mexicanos: diagnóstico, control y tendencias. Ensanut 2020.
Joanne Chang,Gabriella Anic,Brian Rostron,Manju Tanwar,Cindy Chang (2021). Cigarette Smoking Reduction and Health Risks: A Systematic Review and Meta-analysis.
Haiyan Chen,Xiaohua Liang,Li Chen,Lei Zuo,Kuncai Chen,Yuehong Wei,Shouyi Chen,Guang Hao (2022). Associations Between Household Pesticide Exposure, Smoking and Hypertension.
Qihao Chen,Xuxi Ma,Yan Geng,Jingling Liao,Lu Ma (2022). Association between smoking and hypertension under different PM2.5 and green space exposure: A nationwide cross-sectional study.
Grace Falk,Hayrettin Okut, Ph.D.,Mohinder R. Vindhyal, M.D., M.Ed.,Elizabeth Ablah, Ph.D., Mph (2022). Hypertension and Cardiovascular Diseases among Electronic and Combustible Cigarette Users.
Janelle Guirguis-Blake,Corinne Evans,Elizabeth Webber,Erin Coppola,Leslie Perdue,Meghan Weyrich (2021). Screening for Hypertension in Adults.
Ana Herrera,María Corvalán (2017). Tabaquismo en el adolescente.
Robert Kaplan,Pedro Baldoni,Garrett Strizich,Eliseo Pérez-Stable,Nancy Saccone,Carmen Peralta,Krista Perreira,Marc Gellman,Jessica Williams-Nguyen,Carlos Rodriguez,David Lee,Martha Daviglus,Gregory Talavera,James Lash,Jianwen Cai,Nora Franceschini (2021). Current Smoking Raises Risk of Incident Hypertension: Hispanic Community Health Study–Study of Latinos.
Benjamin Kuntz,Lars Kroll,Jens Hoebel,Maria Schumann,Johannes Zeiher,Anne Starker,Thomas Lampert (2018). Zeitliche Entwicklung berufsgruppenspezifischer Unterschiede im Rauchverhalten von erwerbstätigen Männern und Frauen in Deutschland.
J Levenson,A Simon,F Cambien,C Beretti (1987). Cigarette smoking and hypertension. Factors independently associated with blood hyperviscosity and arterial rigidity..
Londoño Pérez,C,Rodríguez Rodríguez,I Andrés,C Díaz,G (2011). Cuestionario para la clasificación de consumidores de cigarrillo (C4) para jóvenes.
Q Lu,E Gottlieb,S Rounds (2018). Effects of cigarette smoke on pulmonary endothelial cells.
J Markidan,J Cole,C Cronin,J Merino,M Phipps,M Wozniak,S Kittner (2018). Smoking and risk of ischemic stroke in young men.
T Nagao,K Nogawa,K Sakata,H Morimoto,K Morita,Y Watanabe,Y Suwazono (2021). Effects of Alcohol Consumption and Smoking on the Onset of Hypertension in a Long-Term Longitudinal Study in a Male Workers' Cohort.
Otto Ruokolainen,Tommi Härkänen,Jouni Lahti,Ari Haukkala,Markku Heliövaara,Ossi Rahkonen (2021). Association between educational level and smoking cessation in an 11-year follow-up study of a national health survey.
Ciaran Scallan,Robert Doonan,Stella Daskalopoulou (2010). The Combined Effect of Hypertension and Smoking on Arterial Stiffness.
Hangchuan Shi,Adam Leventhal,Qiang Wen,Deborah Ossip,Dongmei Li (2023). Sex Differences in the Association of E-cigarette and Cigarette Use and Dual Use With Self-Reported Hypertension Incidence in US Adults.
Lei Wu,Shanshan Yang,Yao He,Miao Liu,Yiyan Wang,Jianhua Wang,Bin Jiang (2016). Association between passive smoking and hypertension in Chinese non-smoking elderly women.
Zuxiang Wu,Yingxing Wu,Jingan Rao,Huan Hu,Chenxi Wang,Ji Wu,Yumeng Shi,Yang Fu,Xiaoshu Cheng,Ping Li (2022). Associations among vitamin D, tobacco smoke, and hypertension: A cross-sectional study of the NHANES 2001–2016.
Y Zhang,Y Feng,S Chen,S Liang,S Wang,K Xu,D Ning,X Yuan,H Zhu,H Pan,G Shan (2021). Relationship between the duration of smoking and blood pressure in Han and ethnic minority populations: a cross-sectional study in China.
Bin Zhao,Jing Li,Luqi Zhang,Jie Liu,Di Feng,Xiaoran Hao,Yun Li,Xian Li,Junqin Ding,Laiyou Li,Lanfeng Li,Xiaohua Yin,Wei Cui (2023). Prevalence of smoking among nurses and its association with blood pressure: A cross‐sectional study in 11 cities of China.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Sarahi Irasema Perez Vazquez. 2026. \u201cThe Impact of Smoking on Systemic Arterial Hypertension in the Latin American Population\u201d. Global Journal of Medical Research - F: Diseases GJMR-F Volume 24 (GJMR Volume 24 Issue F1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.



































































