## I. INTRODUCTION
Schizophrenia (SZ) is a serious and complex mental disorder that affects around $1\%$ of the world's population, causing damage to the patient and family, of multifactorial origin [1]. Its diagnosis involves a set of signs and symptoms and impaired professional or social functioning [2]. Its symptoms affect perception, thought, affect, and behavior [3] without any pathognomonic symptoms [2] and involve distortions of perception about oneself and with external reality [1]. Two or more of the following symptoms are required for diagnosis: delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, and negative symptoms such as diminished emotional expression or avolition, with at least one of the symptoms being the first three [3]. Social anxiety (SA) or social phobia is not included among the necessary symptoms, but is frequent before the onset of the disorder [1] and can represent both a residual and a complication of the illness, contributing to great personal suffering and functional impairment after the acute phase of SZ.
SA can be defined by intense or heightened fear or anxiety of one or more social events in which the person is exposed to the likely evaluation of other individuals [2], as a result of negative assessment [2,4], the possibility of judgment or rejection [4]. It is an interpersonal, intrapersonal, and social system disorder, with impaired reciprocal interaction and communication, such as failure of social cohesion and rejection, emotional and physical feelings such as nervousness and sweating, avoidance attitude of feared situations, and dysfunctional beliefs in social situations or imagining these events [5]. Fear, anxiety or avoidance in people with SA, or social phobia imply clinically significant distress or impairment in social, occupational, or other essential spheres of functioning [2].
Several peripheral markers derived from blood count have been increasingly used as an indirect measure of inflammatory activity in the brain in psychiatric disorders [6-10], calculated under simple laboratory exams [10], from a complete blood count [6,11-13].
The neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR) and platelet-to-lymphocyte ratio (PLR) have been investigated as clinical circulating markers of chronic inflammation in many diseases [9,10,14-17], especially NLR [7,8,18] which constitutes baselines of the innate (neutrophil) and adaptive (lymphocyte) immune systems [6,19,20] and may be less affected by confounding variables, being an effective biomarker to identify patients who may benefit from pharmacological treatment adjuvant anti-inflammatory [6] and therefore more reliable in severe mental disorders [10,19].
Many authors cite the hypothesis of frequent inflammation in SZ [6,7,9,10,17,18], both in pathogenesis [7,9] and pathophysiology [18], where the lymphocyte count was lower and that of neutrophils considered higher in schizophrenics patients [7,9,17].
Moreover, a new index, defined as the systemic immune-inflammation index (SII), based on the count of lymphocytes, neutrophils and platelets [13,16,21,22], has been considered a good index [22], and even a better index to reflect local immune response and systemic inflammation, as its high predictive value has been confirmed in a variety of tumors [13,22], brain infarction, cardiovascular disease, and acute pancreatitis [13].
In addition, there may be a connection between anxiety disorders and inflammation, in which the immune system and inflammation play a role. It is suggested the values of NLR [6,23], MLR and PLR are significantly higher in this disorder, even with a limited number of studies [22]. Despite these two independent observations of increased inflammatory markers in SZ and SA, there are no studies, as long we identified, addressing comorbid SZ-SA and checking if the simultaneous SZ-SA diagnosis may reveal increased inflammation.
## II. OBJECTIVE
Assess the association between social anxiety (SA) and inflammation in patients diagnosed with schizophrenia (SZ), measuring primarily the NLR, and secondarily the SII, MLR and PLR.
## III. METHODS
It's about a cross-sectional study of the association between comorbid AS in SZ and levels of peripheral markers of inflammation, especially NLR.
The first hypothesis is the increased inflammation (revealed by increased NLR) in patients with comorbid SZ-SA compared to patients with SZ without SA. The second hypothesis is that the other markers (SII, MLR and PLR) are also altered in schizophrenics patients with SA than without SA.
The sample comprised 82 patients attending the schizophrenia outpatient clinic of a major teaching hospital in southern Brazil (Hospital de Clínicas de Porto Alegre-HCPA) under the Public Health System, diagnosed with schizophrenia of both genders and aged between 18-70 years. Patients with other psychiatric diagnoses, active or chronic inflammatory or autoimmune diseases, and under treatment with anti-inflammatory or immunosuppressive medication were excluded.
All participants were aware of the research objectives and received an invitation to participate.
Those who agreed to contribute to the study signed the Informed Consent Form (ICF) approved by the Ethics Committee of the HCPA. Patient's medical records were also accessed and consulted to ascertain the information needed for the study.
### a) Instruments
Lieberowitz Social Anxiety Scale (LSAS): developed in 1987 by Michel Liebowitz and translated, adapted and validated in four languages [23]. It is a 24-item questionnaire that assesses fear/anxiety and avoidance in specific social situations [24] with 11 items related to social interaction and 13 items related to public performance [25]. Four-point scale ranging from $0 =$ none to $3 =$ severe, and the total score is obtained by adding the fear and avoidance columns [24,26]. As for the classifications of the scores, there is no consensus in the literature. We based ourselves on the Brazilian study by Dos Santos et al. [23] mentions 32 as a good value for the cut-off point, so we followed the following classification: mild social phobia (32-43 points), moderate (44-81) and severe (from 82 points).
Brief Psychiatric Rating Scale (BPRS): developed by Overall and Gorham, is one of the most widely used scales in psychiatric research; where it originally consisted of 16 items, but in 1966 had two additional things (arousal and disorientation), the BPRS-18 [27]. It is a 7-point Likert scale score, where $0 =$ absent, $1 =$ normal, $2 =$ borderline illness, $3 =$ mild illness, $4 =$ moderately ill, $5 =$ markedly ill, $6 =$ severely ill and $7 =$ extremely ill. The cut-off score for the remission of schizophrenia on the BPRS-6 was less than 5, while the ranges for mild, moderate, and severe severity were 5-9, 10-19, and greater than 20, respectively [28]. Some studies address the domains/dimensions of this scale [29-31], we based ourselves on that of Van Dorn et al. [31]for the following classification: positive domain (items ideas of grandeur, distrust, hallucinatory behavior, and altered thought content), negative (affective withdrawal, psychomotor retardation, and blunted affect), affective (somatic worry, anxiety, feelings of guilt, depressed mood, and hostility), and cognitive disorganization (conceptual disorganization, tension, mannerisms and posture, lack of cooperation, excitement, and disorientation).
Generalized Anxiety Disorder Scale (GAD-7): is a 4-point Likert scale (0-3) ranging from "never" to "every "day", asking how often the patient was bothered. The index is obtained by summing the scores, with cut-off points 5, 10, and 15 allowing the classification of anxiety into none/normal (0-4), mild (5-9), moderate (10-14), and severe (15-21) [32].
Blood count: through a blood test of the patient, to measure biomarkers of inflammation. The complete blood count is routinely collected at the outpatient clinic and included in patients' charts. Some patients have their CBC performed elsewhere, and the patient or family member is asked to access it (we had eight cases in these conditions).
### b) Statistical Analysis
Data analysis was performed using the Statistical Package of Social Science (SSP) software version 27.0, where 82 individuals were analyzed. A descriptive analysis was made of the clinical and sociodemographic characteristics of the total sample and both groups, shown as mean and standard deviation or frequency and percentage. Quantitative variables (inflammation markers, age, time of diagnosis of schizophrenia, number of psychiatric hospitalizations) were described using the mean and standard deviation or median and interquartile range. Categorical variables (gender, family income, education, scales, medications, comorbidities) were described by absolute frequencies and percentages.
The t-student test was used to compare means between the groups with social anxiety and without social anxiety. In the case of asymmetry, the Mann-Whitney test was applied. Pearson's chi-square or Fisher's exact tests were used to compare proportions. Spearman's correlation coefficient was applied to evaluate the correlations between the inflammation markers and the scales under study. Wilcoxon's test was used to compare Liebowitz Scale items about fear and avoidance and between performance and social anxieties. The significance level adopted was $5\%$ $(p < 0.05)$.
To control for possible confounding variables, multivariate Poisson Regression analysis was used to assess factors independently associated with social anxiety. The criterion for entering the variable in the model was that it had a p-value $< 0.20$ in the bivariate analysis. The standard for remaining in the final model was that it had a p-value $< 0.10$. The effect measure used was the Prevalence Ratio (PR) and the $95\%$ confidence interval.
### c) NLR, SII, PLR, and MLR values
There are several studies of typical values for NLR, such as that of Forget [15], in the Belgian adult, non-geriatric population with good health status (between 0.78 and 3.53); Iranian population (NLR $1.70 \pm 0.70$, MLR $11.15 \pm 3.14$ and PLR $117.05 \pm 47.73$, respectively[12]); Chinese (NLR 18-65 years old female $= 0.85 - 3.06$ and male $= 0.90 - 2.94$, PLR 61-179, MLR female $(0.10 - 0.32)$ and male $(0.12 - 0.35)$ and IIS $(161 - 761)[16]$; IIS had a cut-off value of 679.96 (Adali etal. [36]) in research in Turkey.
Cut-off points for patients with squamous cell carcinoma of the external auditory canal with and without preoperative recurrence and those considered ideal were $3.75 \times 109 / L$ for neutrophil count, $1.77 \times 109 / L$ for lymphocyte count, 2.325 for NLR, 157.9 for PLR, and 3.065 for LMR[34]. Szor[35] studied the
Brazilian population, with the cut-off value for NLR was 2.44; Eyff et al.[36] also studied Brazilian adults, with cut-off points for NLR and PLR of 2.80 and 362, respectively.
For the present study, we used the following cut-off points: 2.80 for NLR, 761 for SII, 0.35 for MLR, and 362 for PLR.
## IV. RESULTS
### a) Sample Specifics
As shown in the flowchart in Figure 1, 140 patients were screened and 45 patients were excluded, 15 of these because the electronic medical records did not show a diagnosis of schizophrenia, 06 because they were in the telemedicine care modality, and 24 because they did not accept to participate in the research.
We interviewed 95 patients and excluded 13 patients, 10 of them because they presented other diagnoses (schizoaffective disorder, bipolar disorder, autism, acute psychotic disorder, psychosis due to cognitive disease, organic personality disorder) and 03 patients because of missing information and did not answer all the scales.
As a result, the sample ended up comprising 82 patients, 61 of whom (74.4%) were men and 21 (25.6%) women. The mean age was 47.3 years, and the most frequent schooling was complete high school (47.6%), followed by entire elementary school (32.9%).
As for the clinical characteristics, the mean ages of onset and duration of schizophrenia were 21.9 years and 25.4 years, respectively. The median number of psychiatric hospitalizations was two. The frequency of patients with comorbidities was $79.3\%$, and the main comorbidities found in these patients were obesity $(28\%)$, dyslipidemia $(17.1\%)$, smoking $(15.9\%)$, and diabetes $(14.6\%)$. Most patients were being treated with Clozapine $(96.3\%)$ and $31.7\%$ were using other antipsychotics. The other most used drugs were Clonazepam $(37.8\%)$ and Amitriptyline $(12.2\%)$.
There were no significant differences in all variables between the groups with SA and without SA $(p > 0.050)$.
### b) Social anxiety in schizophrenia
In the present investigation, of the 82 patients meeting the inclusion criteria, 59 patients (72%) had AS comorbidity, with scores higher from 32 in the LSAS, 12.2% being at a mild level of AS, 29.3% moderate, and 30.5% severe.
To complement the study, generalized anxiety was calculated in these patients using the GAD-7 scale, in which $32.9\%$ of patients were at a mild level, $26.8\%$ moderate and $7.3\%$ severe. On the BPRS scale, the classification of the groups was $8.5\%$, $31.7\%$ and $54.9\%$ in mild, moderate and severe scores, respectively.
### c) Social anxiety and inflammation in schizophrenia
The descriptive statistical analysis with the prevalence of the scores of the scales and markers of inflammation (CBC) in the total sample can be seen in Table 1. There was a significant difference in NLR, with $42.7\%$ above the estimated cut-off point. There were also changes in the MLR $(30.5\%)$ and SII $(25.6\%)$, with no changes in the PLR $(0.0\%)$. It is also noted that in addition to $72\%$ of patients showing SAD, $67.1\%$ also had generalized anxiety.
The correlations between the LSAS, GAD-7, and BPRS scales with the inflammation markers NLR, SII, MLR, and PLR are shown in Table 2. There was a statistically significant positive correlation between the LSAS and the NLR, SII, and PLR markers, and the higher the SA scores, the higher the values of these markers; there was no correlation with MLR $(p > 0.50)$, as can also be seen in Figures 2 to 4. No correlation was also obtained between the GAD-7 and BPRS scales with inflammation markers.
It was It was observed an association of increased GAD-7 and BPRS with increased NLR only in patients with comorbid SA (LSAS score $\geq 32$ points) (Table 3), and a trend of MLR and IIS failing to reach statistical significance. There were no PLR altered levels.
After adjustment by the multivariate model (table 4), the following variables remained significantly and independently associated with SA: GAD7 ≥ 5 points $(p = 0.029)$, positive, cognitive disorganization, and total domains of the BPRS $(p = 0.003$, $p = 0.004$ and $p = 0.001$, respectively) and NLR ≥ 2.80 $(p < 0.001)$.
Patients who score five points or more on the GAD-7 scale, i.e. who show generalized anxiety at some level, have a $53\%$ higher prevalence of AS compared to those who score less than five points (no generalized anxiety), regardless of BPRS and NLR.
Patients with one point more in the Positive and Cognitive Disorganization domains of the BPRS have a $4\%$ growth in the prevalence of SA. As for the total score of this same scale, the increase is $2\%$, regardless of GAD-7 and NLR scores.
Finally, patients with an NLR equal to or greater than 2.80, which is the cut-off point, show a $55\%$ increase in the prevalence of AS when compared to those with scores below 2.80 (no change in NLR), regardless of the GAD-7 and BPRS scales.
## V. CONCLUSION
Social anxiety in schizophrenia arises from the difficulty of understanding social situations, where the person does not distinguish the intentions of others. Although it is not primary but secondary to the disease, it promotes excellent harm and disability in these patients, even with stabilized psychosis.
As shown above, we found the prevalence of $72\%$ of SA in patients diagnosed with schizophrenia attending HCPA outpatient clinic. NLR was significantly higher in patients with comorbid SA compared to schizophrenic patients without this condition.
It was observed the severity of schizophrenia symptoms was associated with increased frequency of SA, with patients with SA with increased BPRS and GAD-7 scores. There also appeared to be a greater degree of inflammation in schizophrenia patients with SA, specially NLR, with increased SA scores associated with increased NLR, SII, and PLR (and no association with MLR).
Our findings support previous studies of increased inflammation in schizophrenia and provide new evidence that comorbid SA in people with schizophrenia is linked to increased inflammatory indices. However the design cannot tell us about causality.
In addition to the link between markers of inflammation and social anxiety in patients with schizophrenia, we saw that NLR interferes with SA and this is independent of schizophrenia.
Finally, since the analyzed factors were independence, we concluded that SA depends on the degree of schizophrenia and generalized anxiety, and inflammation caused by increased NLR and that these factors predict SA.
These findings become critical in thinking about new forms of treatment, addressing disability and impairment by social anxiety, with complementary therapies addressing inflammation that may modify the course and prognosis of the disease.
The results of these analyses may be limited by the modest sample size, but even so the results seem to have been significant. Not to mention the patients were interviewed by trained professionals and are being monitored by a team of residents and professors at the outpatient clinic where they have already been diagnosed.
### ACKNOWLEDGEMENTS
The study received research funding from Clinics Hospital of Porto Alegre (HCPA) and Federal University of Rio Grande do Sul (UFRGS).
Disclosure
The authors report no conflicts of interest.
Table 1: Descriptive statistics and prevalences of altered instruments and inflammation markers (blood count = CBC) Table 2: Correlation between the LSAS, GAD-7 and BPRS scales with the inflammation markers NLR, SII, MLR and PLR, through Spearman's correlation coefficient.
<table><tr><td>Variables</td><td>Mean ± DP ou
Median (P25 – P75)</td><td>n (%)</td></tr><tr><td>LSAS</td><td>54 (26,8 – 86,0)</td><td></td></tr><tr><td>≥ 32 points</td><td></td><td>59 (72,0)</td></tr><tr><td>GAD-7</td><td>7 (3 – 11)</td><td></td></tr><tr><td>≥ 5 points</td><td></td><td>55 (67,1)</td></tr><tr><td>BPRS</td><td>21,5 (13 – 30,3)</td><td></td></tr><tr><td>≥ 5 points</td><td></td><td>78 (95,1)</td></tr><tr><td>BLOOD COUNT</td><td></td><td></td></tr><tr><td>Neutrophils</td><td>4,98 ± 2,05</td><td></td></tr><tr><td>Monocytes</td><td>0,59 ± 0,21</td><td></td></tr><tr><td>Lymphocytes</td><td>2,05 ± 0,76</td><td></td></tr><tr><td>Platelets</td><td>215,4 ± 65,5</td><td></td></tr><tr><td>Neutrophil-lymphocyte ratio</td><td>2,50 (1,50 – 3,49)</td><td></td></tr><tr><td>≥ 2,80</td><td></td><td>35 (42,7)</td></tr><tr><td>Monocyte-lymphocyte ratio</td><td>0,29 (0,22 – 0,37)</td><td></td></tr><tr><td>≥ 0,35</td><td></td><td>25 (30,5)</td></tr><tr><td>Platelet-lymphocyte ratio</td><td>108,1 (82,8 – 143,5)</td><td></td></tr><tr><td>≥ 362</td><td></td><td>0 (0,0)</td></tr><tr><td>Systemic immune-inflammatory index</td><td>535 (303,5 – 794,2)</td><td></td></tr><tr><td>≥ 761</td><td></td><td>21 (25,6)</td></tr></table>
LSAS = Liebowitz Social Anxiety Scale; BRPS = Brief Psychiatric Rating Scale; GAD-7 = Generalized Anxiety Disorder Scale; NLR = Neutrophil-to-Lymphocyte Ratio; SII = Systemic Immune-Inflammatory Index; MLR = Monocyte-to-Lymphocyte Ratio; PLR = Platelet-to-Lymphocyte Ratio; rs = Spearman's correlation coefficient.
<table><tr><td rowspan="2">Markers of Inflammation</td><td colspan="2">LSAS</td><td colspan="2">GAD-7</td><td colspan="2">BPRS</td></tr><tr><td>rs</td><td>p</td><td>rs</td><td>p</td><td>rs</td><td>P</td></tr><tr><td>NLR</td><td>0,241</td><td>0,029</td><td>0,020</td><td>0,860</td><td>-0,058</td><td>0,606</td></tr><tr><td>SII</td><td>0,257</td><td>0,020</td><td>0,111</td><td>0,321</td><td>-0,054</td><td>0,630</td></tr><tr><td>MLR</td><td>0,110</td><td>0,326</td><td>-0,005</td><td>0,963</td><td>-0,043</td><td>0,702</td></tr><tr><td>PLR</td><td>0,236</td><td>0,032</td><td>0,112</td><td>0,318</td><td>-0,003</td><td>0,982</td></tr></table>
Table 3: Prevalence of alterations in the GAD-7 and BPRS scales and in the blood count according to the LSAS classification
<table><tr><td>Variables</td><td>No AS (n=23; 28%)</td><td>Yes AS (n=59; 72%)</td><td>P</td></tr><tr><td>GAD-7</td><td></td><td></td><td></td></tr><tr><td>≥ 5 points</td><td>9 (39,1)</td><td>46 (78,0)</td><td>0,002</td></tr><tr><td>BPRS</td><td></td><td></td><td></td></tr><tr><td>≥ 5 points</td><td>19 (82,6)</td><td>59 (100)</td><td>0,005</td></tr><tr><td>BLOOD COUNT</td><td></td><td></td><td></td></tr><tr><td>Neutrophil-lymphocyte ratio</td><td></td><td></td><td></td></tr><tr><td>≥ 2,80</td><td>5 (21,7)</td><td>30 (50,8)</td><td>0,032</td></tr><tr><td>Monocyte-lymphocyte ratio</td><td></td><td></td><td></td></tr><tr><td>≥ 0,35</td><td>4 (17,4)</td><td>21 (35,6)</td><td>0,180</td></tr><tr><td>Systemic immune-inflammatory index</td><td></td><td></td><td></td></tr><tr><td>≥ 761</td><td>3 (13,0)</td><td>18 (30,5)</td><td>0,178</td></tr></table>
Table 4: Multivariate Poisson Regression Analysis to assess factors independently associated with social anxiety
<table><tr><td>Variables</td><td>Prevalence Ratio (95% CI)</td><td>P</td></tr><tr><td>GAD-7 ≥ 5 points</td><td>1.53 (1.04 – 2.25)</td><td>.029</td></tr><tr><td>BPRS</td><td></td><td></td></tr><tr><td>Positive Domain</td><td>1.04 (1.01 – 1.06)</td><td>.003</td></tr><tr><td>Disorganized Cognitive Domain</td><td>1.04 (1.01 – 1.07)</td><td>.004</td></tr><tr><td>Total score</td><td>1.02 (1.01 – 1.03)</td><td>.001</td></tr><tr><td>Neutrophil-Lymphocyte Ratio ≥ 2,80</td><td>1.55 (1.21 – 1.98)</td><td><.001</td></tr></table>
 Source: Elaborated by the author.
 Figure 1: PRISMA Flowchart: patients screened, interviewed, excluded, included, eligible. Figure 2: Scatter diagram of LSAS's correlation with NLR.
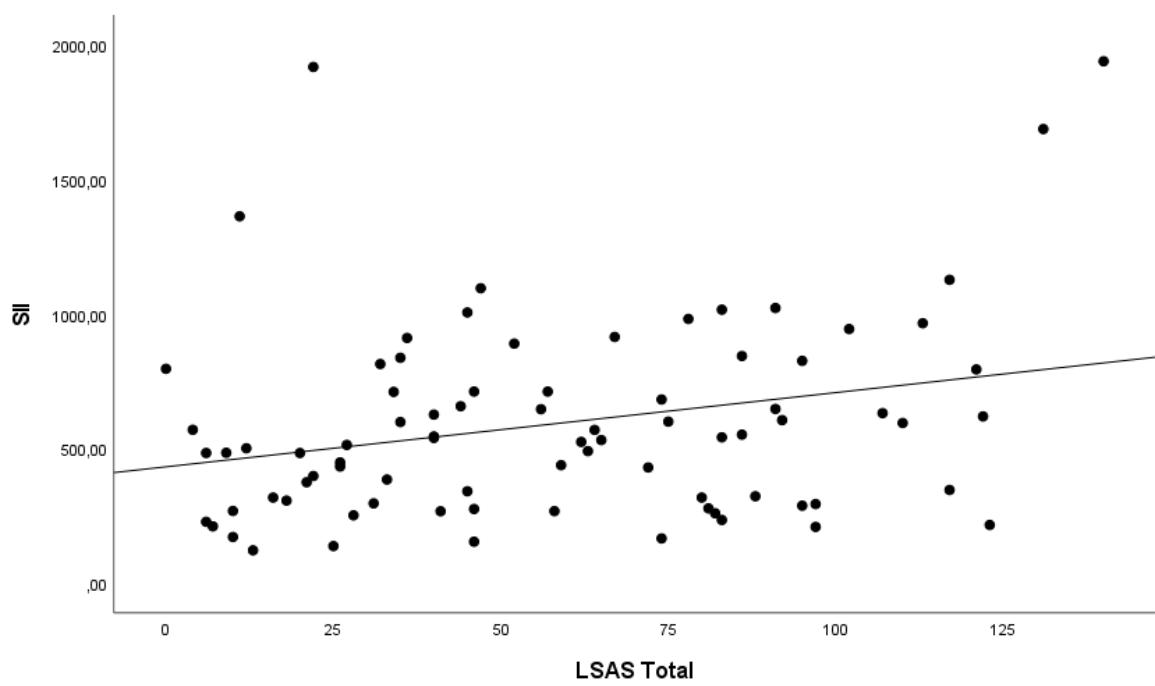 Figure 3: Scatter diagram of the LSAS correlation with SII.
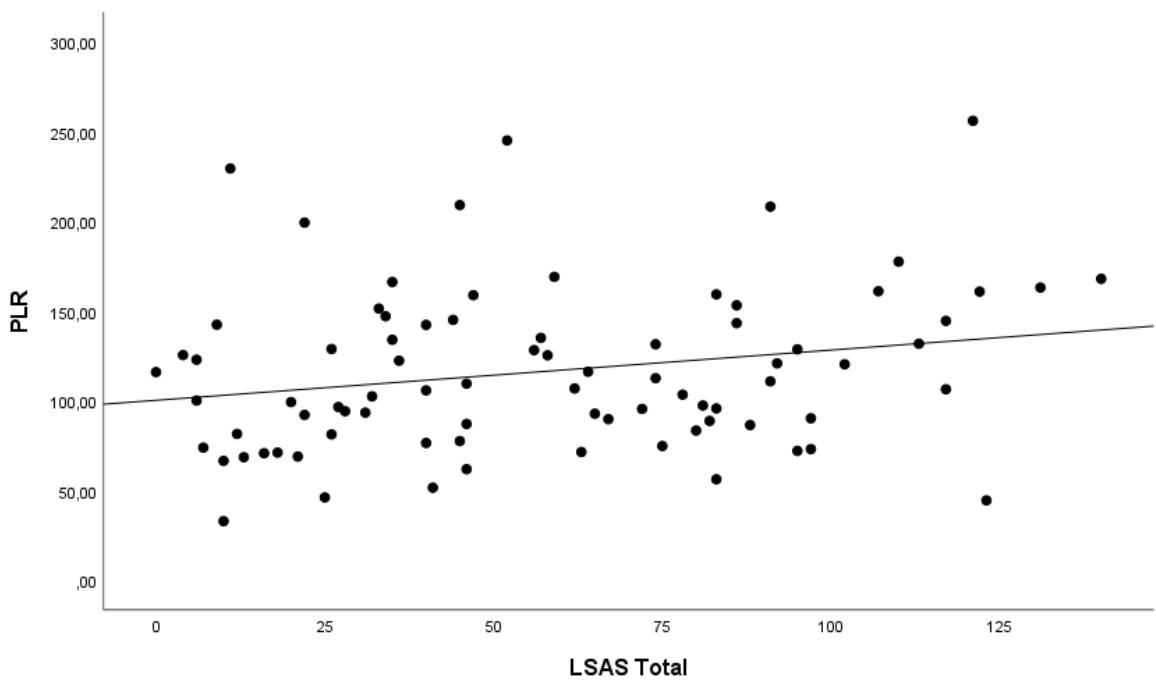 Figure 4: Scatter diagram of the correlation of LSAS with PLR.
Generating HTML Viewer...
References
36 Cites in Article
A Silva,Dos Santos,C Miron,F Miguel,N Furtado,C Bellemo,Ais (2016). Schizophrenia: a literature review.
(2022). Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR).
Maria Ruiz-Iriondo,Karmele Salaberria,Enrique Echeburua,Alvaro Iruin,Olga Gabaldón Poc,Idoia Fernández Marañón (2019). Global functioning among middle-aged patients with chronic schizophrenia: the role of medication, working memory and verbal comprehension.
Stefania Barzeva,Jennifer Richards,Wim Meeus,Albertine Oldehinkel (2020). The social withdrawal and social anxiety feedback loop and the role of peer victimization and acceptance in the pathways.
Christina Hunger,Rebecca Hilzinger,Laura Klewinghaus,Laura Deusser,Anja Sander,Johannes Mander,Hinrich Bents,Beate Ditzen,Jochen Schweitzer (2019). Comparing Cognitive Behavioral Therapy and Systemic Therapy for Social Anxiety Disorder: Randomized Controlled Pilot Trial (<scp>SOPHO</scp>‐<scp>CBT</scp>/<scp>ST</scp>).
A Brinn,J Stone (2020). Neutrophiltolymphocyte ratio in psychiatric diagnoses: a cross-sectional study using electronic health records.
Burak Kulaksizoglu,Sibel Kulaksizoglu (2016). Relationship between neutrophil/lymphocyte ratio with oxidative stress and psychopathology in patients with schizophrenia.
Selçuk Özdin,Ömer Böke (2019). Neutrophil/lymphocyte, platelet/lymphocyte and monocyte/lymphocyte ratios in different stages of schizophrenia.
S Sahin,C Yasamali,M Özyürek,G Elboga,A Altindag,A Sahin (2020). Neutrophil-lymphocyteratio in catatonia.
Yasin Balcioglu,Simge Kirlioglu (2020). C-Reactive Protein/Albumin and Neutrophil/Albumin Ratios as Novel Inflammatory Markers in Patients with Schizophrenia.
M Moosazadeh,I Maleki,R Alizadeh-Navaei,M Kheradmand,A Hedayatizadeh-Omran,A Shamshirian (2019). Normal values of neutrophilto-lymphocyte ratio, lymphocyte-to-monocyte ratio and platelet-to-lymphocyte ratio among Iranian population: Results of Tabari cohort.
Y Wei,T Wang,G Li,J Feng,L Deng,H Xu (2022). Investigation of systemic immune-inflammation index, neutrophil/high-density lipoprotein ratio, lymphocyte/high-density lipoprotein ratio, and monocyte/high-density lipoprotein ratio as indicators of inflammation in patients with schizophrenia and bipolar disorder.
Ikbal Inanli,Memduha Aydin,Ali Çaliskan,Ibrahim Eren (2019). Neutrophil/lymphocyte ratio, monocyte/lymphocyte ratio, and mean platelet volume as systemic inflammatory markers in different states of bipolar disorder.
Patrice Forget,Céline Khalifa,Jean-Philippe Defour,Dominique Latinne,Marie-Cécile Van Pel,Marc De Kock (2017). What is the normal value of the neutrophil-to-lymphocyte ratio?.
Xianchun Meng,Qian Chang,Yuying Liu,Ling Chen,Gaohui Wei,Jingjing Yang,Peiguo Zheng,Fucheng He,Wanhai Wang,Liang Ming (2018). Determinant roles of gender and age on <scp>SII</scp>,<scp> PLR</scp>,<scp> NLR</scp>,<scp> LMR</scp> and <scp>MLR</scp> and their reference intervals defining in Henan, China: A posteriori and big‐data‐based.
Özdinselçuk,G Sarisoy,Ö Böke (2017). A comparison of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratios in schizophrenia and bipolar disorder patients -a retrospective file review.
M Semiz,O Yildirim,F Canan,S Demir,E Hasbek,T Tuman (2014). Elevated neutrophil/lymphocyte ratio in patients with schizophrenia.
R Zahorec (2021). Neutrophil-to-lymphocyte ratio, past, present and future perspectives.
Minkyo Song,Barry Graubard,Charles Rabkin,Eric Engels (2021). Neutrophil-to-lymphocyte ratio and mortality in the United States general population.
Bekir Demiryürek,Esra Demiryürek,Deniz Çekiç,Kubilay İşsever,Ahmed Genç,Selcuk Yaylacı (2022). DEPRESSION AND ANXIETY DISORDERS IN COVID-19 SURVIVORS: ROLE OF INFLAMMATORY PREDICTORS.
Huaping Huang,Qin Liu,Lixia Zhu,Yan Zhang,Xiaojuan Lu,Yawei Wu,Li Liu (2019). Prognostic Value of Preoperative Systemic Immune-Inflammation Index in Patients with Cervical Cancer.
Dos Santos,L (2012). Validity and reliability study of Liebowitz Social Anxiety Scale -self-applied version.
V Caballo,I Salazar,V Arias,S Hofmann,J Curtiss (2019). Psychometric properties of the Liebowitz Social Anxiety Scale in a large cross-cultural Spanish and Portuguese speaking sample.
N Rytwinski,D Fresco,R Heimberg,M Coles,M Liebowitz,S Cissell,M Stein,S Hofmann (2009). Screening for social anxiety disorder with the self-report version of the Liebowitz Social Anxiety Scale.
Necati Uzun,Mehmet Akıncı (2020). Hemogram parameters in childhood anxiety disorders: Could anxiety disorders be related with inflammation?.
J Crippa,R Sanches,J Hallak,S Loureiro,A Zuardi (2002). Factor structure of Bech's version of the Brief Psychiatric Rating Scale in Brazilian patients.
J Crippa,R Sanches,J Hallak,S Loureiro,A Zuardi (2002). Factor structure of Bech's version of the Brief Psychiatric Rating Scale in Brazilian patients.
Seon-Cheol Park,Eun Jang,Kiwon Kim,Hoseon Lee,Joonho Choi,Amitava Dan,Arshad Hussain,Andi Tanra,Takahiro Kato,Kok Chee,Sih-Ku Lin,Chay Tan,Afzal Javed,Norman Sartorius,Naotaka Shinfuku,Yong Park (2019). Establishing the cut-off scores for the severity ranges of schizophrenia on the BPRS-6 scale: findings from the REAP-AP.
Medeiros Hlv De,D Rocha,Rmew Roudig,Amp Silva,Da (2017). Validated schizophrenia assessment scales for use in brazil: a systematic review.
Freitas Rr De (2018). Assessment of Psychopathological Dimensions of treatment-resistant and nontreatment-resistant Schizophrenia: an international multicentercross-sectional study.
Richard Van Dorn,Sarah Desmarais,Kevin Grimm,Stephen Tueller,Kiersten Johnson,Brian Sellers,Marvin Swartz (2016). The latent structure of psychiatric symptoms across mental disorders as measured with the PANSS and BPRS-18.
T Sousa,V Viveiros,M Chai,F Vicente,G Jesus,M Carnot (2015). Reliability and validity of the Portuguese version of the Generalized Anxiety Disorder (GAD-7) scale.
Mehmet Adali,Ipek Buber,Gursel Sen,Samet Yilmaz (2022). Relação entre o Índice Imune-inflamação Sistêmico e Circulação Colateral Coronariana em Pacientes com Oclusão Total Crônica.
F Li,X Shi,C Dai (2022). Prognostic value of pre-operative peripheral inflammation markers in patients with squamous cell carcinoma of the external auditory canal.
Daniel Szor,André Dias,Marina Pereira,Marcus Ramos,Bruno Zilberstein,Ivan Cecconello,Ulysses Ribeiro (2019). Neutrophil-lymphocyte ratio change after curative gastrectomy for gastric cancer: a subgroup analysis.
Tatiana Eyff,Henrique Bosi,Mariana Toni,Mariana Zilio,Carlos Corso,Vivian Bersch,Alessandro Osvaldt (2018). THE ROLE OF IMMUNOINFLAMMATORY MARKERS IN THE PROGNOSIS AND RESECTABILITY OF PANCREATIC ADENOCARCINOMA.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Amelia Dias Teixeira. 2026. \u201cThe link between Social Anxiety and Peripheral Inflammatory Markers in patients with Schizophrenia diagnoses\u201d. Global Journal of Medical Research - A: Neurology & Nervous System GJMR-A Volume 23 (GJMR Volume 23 Issue A3).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.