



I. INTRODUCTION
According to the Global Burden of Oral Conditions of 1990-2010, tooth loss is among the 100 conditions that most impacted humanity, affecting of the world's population[^1]. The progressive increase in tooth loss with advancing age represents the sequela of caries and periodontal disease[^2] and reflects the lack of access to dental services or even the provision of mutilating services[^3]. The absence of teeth can cause impairments in digestion and affect masticatory function, food selection, phonation and facial aesthetics, which favors the development of psychological disorders and has a negative impact on quality of life. In addition, it is related to obesity, cognitive dysfunction and other potentially degenerative conditions such as atherosclerosis and cardiovascular diseases, reflecting on mortality.
National surveys show a high prevalence of tooth loss, especially among the elderly [10], with a recent trend of decrease in all age groups, but mainly among younger people in the last decades [11]. This decrease is attributed to the combination of improvements in socioeconomic conditions, mostly in education, and the implementation of the National Oral Health Policy, which expanded fluoridation of the water supply and disseminated fluoridated toothpastes, among other measures [2,10,12].
However, tooth loss still represents a concern for the health of Brazilian adults and the elderly . This condition may be more worrisome among cancer patients because of the treatment toxicity , their social vulnerability, and their health condition, which can cause oral diseases to be neglected. It should be considered that the incidence of cancer has grown rapidly worldwide, which generates social, general and oral health demands for these groups . According to the National Cancer Institute (INCA), 625,000 new cases of cancer are expected for each year of the triennium 2020-2022 in Brazil .
However, few studies focus on tooth loss in this specific population. From this perspective, the classification of the position of tooth losses used in conjunction with its quantification can contribute to the understanding of this outcome, besides assisting in the identification of important aesthetic and functional issues in the planning of oral rehabilitation of these patients[2,17]. This study was carried out considering the usefulness of a classification of tooth loss according to the number and position of missing teeth to identify social, behavioral and oral health determinants not usually detected by traditional evaluations[18]. Also, it was considered how such information can support the planning, promotion and prevention of oral diseases in a scenario of scarce specific information[^2]. Thus, its objective was to evaluate the prevalence and factors associated with tooth loss, according to the number and position of missing teeth in cancer patients in southern Minas Gerais, Brazil.
II. MATERIAL AND METHODS
a) Ethical Considerations
The procedures used in this study adhere to the tenets of the Declaration of Helsinki and the Resolution 466, December 2012, of the Brazilian National Health Council. The present study was approved by the Research Ethics Committee involving Human Beings of the Federal University of Alfenas (UNIFAL/MG) (CAAE: 40017720.6.0000.5142). In addition, informed written consent was obtained from all participants.
b) Study Design, Scenario and Participants
This study was developed at the facility of a voluntary association for cancer patients in a municipality in southern Minas Gerais, Brazil. It is a nongovernmental organization, active in town since 2002 and recognized as a public utility in several spheres . The population base was of patients assisted by this association and who are undergoing cancer treatment in a philanthropic organization that serves 24 municipalities in two microregions of the State of Minas Gerais, representing a population of approximately 437,005 inhabitants . These patients were invited to participate in the study in 2021, when the epidemiological conditions of SARS-COV-2 pandemic control enabled its realization.
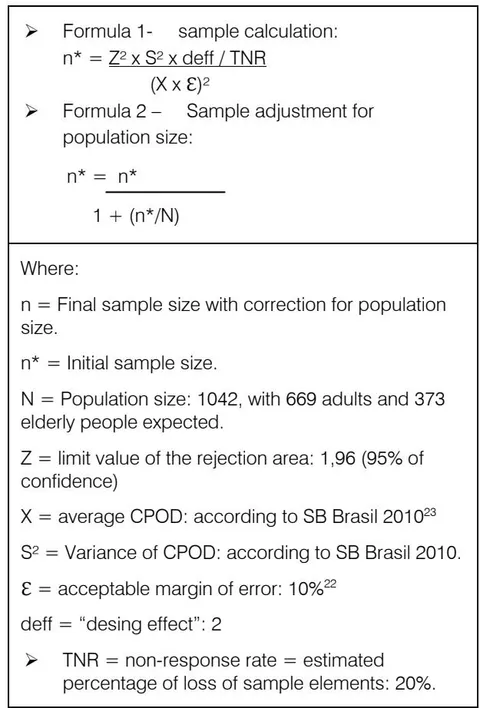
To determine the minimum sample required for the study, a stratified random sampling was obtained and partitioned into two age groups: adults and the elderly. The calculation to obtain the minimum sample was based on a population mean (DMFT for populations between 35-44 and 65-74 years in the interior of Southeastern Brazil), used as a reference for the adult and elderly groups by the WHO and obtained in the last national oral health survey . The formulas used are shown in Chart 1 and follow the standards applied in the SB BRASIL study .
criteria were: having a confirmed diagnosis of cancer, being under cancer treatment, not having communication difficulties that would prevent the interview or the intraoral clinical examination, and being 18 years or older.
c) Variables under Study
The outcome of this study was tooth loss, assessed by intraoral clinical examination performed according to internationally recommended parameters[21,24]. Participants were classified as: (i) having functional dentition (FD) [presence of 20 or more teeth] without anterior losses; (ii) having FD with anterior losses; (iii) having no FD.
The independent variables listed for the analysis were divided into the following blocks: (1) Socioeconomic characteristics; (2) Health-related habits (HRH); (3) General Health; (4) Oral health; (5) Oral alterations after cancer treatment; and (6) Dental care. In (1), the variables incorporated were: age group (18-40/41-59/60-79 / ≥ 80 years); sex; skin color (white and non-white); schooling (0-3/4-7 / ≥ 8 years of study); income (< 1/1-2 / > 2 minimum wages – according to values in 2021); and whether the participant lives with a partner (yes/no). In block (2), the current smoking habit (yes/no); current alcohol intake (yes/no), and physical activity for more than 150 minutes per week (yes/no) were evaluated.
In block (3), we evaluated multimorbidity (presence of two or more synchronous comorbidities to cancer: hypertension, diabetes mellitus, cardiovascular diseases, gastrointestinal problems, and anemia); polypharmacy (the use of four or more medications at the same time in the last three months [yes/no]); time elapsed since cancer diagnosis years); previous experience with any type of cancer (yes/no); location of the tumor in treatment or being followed-up (head or neck/other location); types of cancer treatment already performed: surgery (yes/no), medications (yes/no), chemotherapy (yes/no), and radiotherapy (yes/no). In block (4), the variables were: dental prosthesis (does not use and does not need it/does not use but needs it/uses it); presence of caries (yes/no); calculus (yes/no); gingival bleeding (yes/no); periodontal pockets (yes/no); clinical attachment loss (CAL) (yes/no); poor oral health self-assessment (yes/no), and self-perception of need for dental treatment (yes/no). In block (5), the presence of dry mouth, trismus, painful wounds, dormant areas, feeding alteration, flavor alteration, difficulty speaking, and difficulty swallowing were evaluated. In block (6), the variables evaluated were the frequency of daily tooth brushing (0-2/3 times or more); last dental appointment year); type of dental service used in the last consultation (public/private), and reason for the last dental consultation (pain/others).
Blocks 1, 2, 3, 5 and 6 were collected exclusively through interviews and recorded in a questionnaire. The variables self-assessment of poor oral health and self-perception of the need for dental treatment from block 4 were collected through interviews, but the clinical conditions (tooth loss, dental prosthesis, caries, calculus, bleeding, periodontal pocket and CAL) were evaluated through intraoral physical examination, as recommended by the WHO's basic manual of oral health surveys . All stages of the study were performed in the physical space of the institution by the researchers themselves, who were properly trained and calibrated (kappa inter examiner = 0.98).
d) Data Analysis
Data analysis was performed by estimating absolute and relative frequencies of the variables, in addition to mean age and standard deviation for the entire sample (Table 1). The bivariate analysis of the association between tooth loss and independent variables was performed using Simple Multinomial Logistic Regression models. The reference category was (i). The independent variables that presented a p-value in the bivariate association with the outcome were incorporated into the analysis of multiple variables in the Multiple Multinomial Logistic Regression model. The association estimates were expressed by odds ratio (OR) with confidence intervals. For all procedures, the significance level of was adopted. All analyses were performed using the Stata 14.0 software (Stata Corp LLP, College Station, TX).
III. RESULTS
Table 1 shows a description of the characteristics of the study participants. Mean age was 61.07 (SD 0.61) years. The sample consisted of a majority of women (53.97%), people who had up to 3 years of schooling (71.66%), and who had a family income up to two minimum wages (83.45%). From all participants, 18.68% currently smoke, 12.50% perform at least 150 minutes of physical activity per week, 23.81% have two or more chronic conditions concomitant with cancer, and 15.07% use at least four daily medications in the last three months. Also, 58.09% have been undergoing treatment for more than a year, and 22.68% of patients had a previous experience with cancer. The most and least used types of cancer treatment were medication (59.32%) and radiotherapy (44.55%), respectively. Regarding oral health conditions, 53.14% use and 87.20% require prosthesis. In addition, 23.19% of participants have active caries, 48.55% presented calculus, and 48.31% periodontal pockets. However, only 10.43% consider their oral health to be poor. The most reported oral alterations after cancer treatment were dry mouth (60.36%) and changes in food flavor (43.54%). Almost half (47.17%) of the sample brushes their teeth at least 3 times a day, 66.97% had their last dental appointment more than one year ago, 66.95% sought private dental care, and pain was the reason for the last consultation for 11.11% of interviewees. The outcome of the study showed the following distribution: (i) of participants presented FD without anterior losses; (ii) have FD with anterior losses; and (iii) do not have FD.
Table 2 shows the results of the bivariate analysis of factors associated with tooth loss, analyzed according to the number and location of missing teeth, using group (i) as reference. Individuals with a higher chance of having FD with anterior losses were older individuals , those who had lower income , those who use and those who require prostheses, those who did not report flavor alteration , and individuals whose last dental consultation was performed in the public service .
| Block | Variable | Category | n | % |
| Socioeconomic Conditions | Age group | 18-40 years | 19 | 4,31 |
| 41-59 years | 176 | 39,91 | ||
| 60-79 years | 217 | 49,21 | ||
| 80 ou + years | 29 | 6,58 | ||
| Gender | Women | 238 | 53,97 | |
| Skin color | White | 229 | 52,89 | |
| Schooling | ≤ 3 years of study | 316 | 71,66 | |
| 4-7 years of study | 103 | 23,36 | ||
| ≥ 8 years of study | 22 | 4,99 | ||
| Income | <1 minimum wage | 31 | 7,23 | |
| 1-2 minimum wage | 327 | 76,22 | ||
| >2 minimum wage | 71 | 16,55 | ||
| Lives with partner | Yes | 65 | 14,74 | |
| HRH | Present smoke | Yes | 82 | 18,68 |
| Present alcoholic | Yes | 80 | 18,14 | |
| Physical activity | >150 min./week | 55 | 12,50 | |
| General Health | Multimorbidity | ≥2 chronic conditions | 105 | 23,81 |
| Polypharmacy | ≥4 drug | 66 | 15,07 | |
| Cancer time | 2 ou + Years | 255 | 58,09 | |
| Previous cancer experience | Yes | 100 | 22,68 | |
| Tumor time | Head/neck | 34 | 7,71 | |
| Surgical treatment | Yes | 249 | 56,72 | |
| Drug treatment | Yes | 261 | 59,32 | |
| Chemotherapy | Yes | 251 | 57,05 | |
| Radiotherapy | Yes | 196 | 44,55 | |
| Oral health | Tooth loss | FD, no loss front | 113 | 27,29 |
| FD, with loss front | 25 | 6,04 | ||
| No FD | 276 | 66,67 | ||
| Dental prosthesis | Not use and not need it | 51 | 12,32 | |
| Not use but need | 143 | 34,54 | ||
| Use | 220 | 53,14 | ||
| Caries | Yes | 96 | 23,19 | |
| Calculus | Yes | 201 | 48,55 | |
| Gingival bleeding | Yes | 108 | 26,09 | |
| Peiodontal pocket | Yes | 200 | 48,31 | |
| Periodontal attachment loss | Yes | 153 | 36,96 | |
| Oral health bad | Yes | 46 | 10,43 | |
| Self perception treatment | Yes | 239 | 54,20 | |
| Oral changes after cancer treatment | Dry mouth | Yes | 265 | 60,36 |
| Trismus | Yes | 54 | 12,24 | |
| Wound | Yes | 151 | 34,32 | |
| Dornant áreas | Yes | 28 | 6,35 | |
| Food change | No | 187 | 42,50 | |
| Yes, decrease | 182 | 41,36 | ||
| Yes, increase | 71 | 16,14 | ||
| Flavor change | Yes | 192 | 43,54 | |
| Difficulty speaking | Yes | 53 | 12,02 | |
| Difficulty swallow | Yes | 83 | 18,82 | |
| Brushing frequency 3vz ou + | Yes | 208 | 47,17 | |
| Dental care | Last dental appointment more than 1 year ago | Yes | 294 | 66,97 |
| Private used service | Yes | 292 | 66,95 | |
| Reason for last consultation pain | Yes | 49 | 11,11 |
The chances of not having FD were higher among older individuals , men , less educated individuals , those with lower income , those who do not ingest any amount of alcoholic beverages , those with multimorbidities and polypharmacy , patients who underwent chemotherapy , and those who use and require prostheses. Also, among individuals without caries , without calculus , without bleeding , without periodontal pocket , without clinical attachment loss , those who did not report flavor alteration , those who had no change in food intake when compared to those who increased food intake , those who brush their teeth less than three times a day , those who attended their last dental appointment more than one year ago , and those whose reason for the last visit was different from pain .
Table 3 shows the results of the adjusted multiple analysis of factors associated with tooth loss. The individuals with higher chances of having FD with anterior losses were those who have an income lower than one minimum wage (when compared to individuals with an income higher than two salaries, ) and individuals who did not report flavor alteration after the beginning of their cancer treatment ( ), regardless of their socioeconomic situation, general and oral health. Subjects more likely not to have FD were older individuals ( ), less educated individuals ( ), those who use prostheses ( ), those without periodontal pockets ( ), and those who brush their teeth less than three times a day ( ), regardless of socioeconomic situation, general and oral health.
| Variable | FD with front loss | No FD | ||||||
| OR | IC 95% | p | OR | IC 95% | p | |||
| Socioeconomic Conditions | Age group | 1,04 | 1,00-1,08 | 0,032 | 1,11 | 1,09-1,14 | <0,001 | |
| Gender (ref.: masculino) | Feminine | 1,11 | 0,44-2,82 | 0,810 | 0,47 | 0,30-0,75 | 0,001 | |
| Skin color (ref.: no white) | White | 0,61 | 0,26-1,48 | 0,282 | 0,66 | 0,42-1,04 | 0,075 | |
| Schooling (ref.: <3 anos) | 4-7 year | 0,65 | 0,27-1,59 | 0,350 | 0,16 | 0,09-0,27 | <0,001 | |
| ≥8 year | 0,01 | 0,00-∞ | 0,980 | 0,90 | 0,03-0,25 | <0,001 | ||
| Income (ref.: <1 sal min) | 1-2 | 0,61 | 0,10-3,56 | 0,584 | 0,49 | 0,16-1,46 | 0,201 | |
| >2 | 0,05 | 0,00-0,75 | 0,030 | 0,14 | 0,04-0,46 | 0,001 | ||
| Partner (ref.: no) | Yes | 0,47 | 0,15-1,50 | 0,204 | 0,84 | 0,42-1,69 | 0,638 | |
| HRH | Present smoke (ref.: no) | Yes | 1,61 | 0,52-4,96 | 0,401 | 1,76 | 0,95-3,27 | 0,070 |
| Present alcoholic(ref.: no) | Yes | 0,87 | 0,31-2,39 | 0,793 | 0,46 | 0,27-0,80 | 0,006 | |
| Physical activity (ref.: <150min) | ≥150min. | 1,76 | 0,61-5,06 | 0,290 | 0,70 | 0,37-1,34 | 0,286 | |
| General Health | Multimorbidity (ref.: no) | Yes | 2,42 | 0,82-7,18 | 0,109 | 2,97 | 1,57-5,61 | 0,001 |
| Polypharmacy (ref.: no) | Yes | 2,5 | 0,69-9,06 | 0,163 | 2,83 | 1,28-6,13 | 0,010 | |
| Diagnosis (ref.: <2 years) | ≥2 years | 2,30 | 0,89-5,96 | 0,084 | 1,30 | 0,84-2,03 | 0,235 | |
| Cancer experience (ref.: no) | Yes | 0,67 | 0,21-2,13 | 0,499 | 1,17 | 0,69-1,97 | 0,548 | |
| Surgical treat. (ref.: no) | Yes | 0,87 | 0,36-2,08 | 0,761 | 1,08 | 0,69-1,69 | 0,706 | |
| Drug treat. (ref.: no) | Yes | 1,43 | 0,58-3,52 | 0,432 | 1,18 | 0,75-1,83 | 0,462 | |
| Chemotherapy(ref.: no) | Yes | 0,70 | 0,28-1,75 | 0,448 | 0,44 | 0,27-0,70 | 0,001 | |
| Radiotherapy (ref.: no) | Yes | 1,14 | 0,48-2,72 | 0,761 | 1,02 | 0,66-1,59 | 0,908 | |
| Oral care | Tooth loss (ref.: no) | Yes | 5,4 | 1,43-20,38 | 0,013 | 68,72 | 26,8-175,6 | <0,001 |
| Dental prosthesis (ref.: no) | Yes | 3,87 | 1,25-12,03 | 0,019 | 203,07 | 27,5-1498,5 | <0,001 | |
| Caries (ref.: no) | Yes | 2,33 | 0,96-5,66 | 0,060 | 0,58 | 0,35-0,98 | 0,040 | |
| Calculus (ref.: no) | Yes | 6,47 | 0,83-50,30 | 0,074 | 0,12 | 0,07-0,21 | <0,001 | |
| Gingival bleeding (ref.: no) | Yes | 2,23 | 0,92-5,37 | 0,073 | 0,42 | 0,25-0,68 | <0,001 | |
| Periodontal pocket (ref.: no) | Yes | 1,29 | 0,35-4,82 | 0,696 | 0,07 | 0,04-0,13 | <0,001 | |
| Periodontal loss (ref.: no) | Yes | 1,31 | 0,53-3,22 | 0,552 | 0,26 | 0,16-0,41 | <0,001 | |
| SB bad (ref.: good) | Bad | 1,78 | 0,44-7,29 | 0,417 | 1,60 | 0,71-3,60 | 0,257 | |
| Self perception treat. (ref.: no) | Yes | 2,42 | 0,90-6,53 | 0,080 | 0,83 | 0,54-1,30 | 0,423 | |
| Variable | FD with front loss | No FD | ||||||
| OR | IC 95% | p | OR | IC 95% | p | |||
| Oral changes after cancer treatment | Dry mouth (ref.: no) | Yes | 1,52 | 0,58-3,94 | 0,388 | 0,88 | 0,56-1,38 | 0,586 |
| Trismus (ref.: no) | Yes | 0,61 | 0,13-2,90 | 0,538 | 1,06 | 0,55-2,05 | 0,861 | |
| Wound (ref.: no) | Yes | 1,76 | 0,74-4,21 | 0,202 | 0,81 | 0,52-1,29 | 0,388 | |
| Dorment area (ref.: no) | Yes | 1,55 | 0,29-8,17 | 0,605 | 1,31 | 0,51-3,39 | 0,566 | |
| Food change (ref.: no) | Decrease | 0,77 | 0,30-1,99 | 0,600 | 0,89 | 0,55-1,46 | 0,658 | |
| Increase | 0,404 | 0,10-1,57 | 0,190 | 0,47 | 0,26-0,88 | 0,018 | ||
| Flavor change (ref.: no) | Yes | 0,40 | 0,16-0,98 | 0,046 | 0,44 | 0,28-0,70 | <0,001 | |
| Difficulty speaking (ref.: no) | Yes | 0,89 | 0,18-4,36 | 0,892 | 1,59 | 0,76-3,32 | 0,214 | |
| Difficulty swallow (ref.: no) | Yes | 0,78 | 0,24-2,52 | 0,689 | 0,98 | 0,56-1,71 | 0,952 | |
| Dental care | Brushing (ref.: no) | 3vz ou + | 0,52 | 0,22-1,27 | 0,153 | 0,30 | 0,19-0,48 | <0,001 |
| Last consult (ref.: < 1 year) | ≥1 year | 0,74 | 0,31-1,78 | 0,508 | 0,31 | 0,19-0,49 | <0,001 | |
| Service private (ref.: public) | Private | 0,29 | 0,12-0,70 | 0,006 | 0,71 | 0,44-1,16 | 0,179 | |
| Reason for last consult pain (ref.: no) | Yes | 0,56 | 0,15-2,05 | 0,385 | 0,36 | 0,19-0,68 | 0,002 | |
| Variable | With functional dentition but anterior loss | No Functional Dentition | ||||||
| OR | IC95% | p | OR | IC95% | p- | |||
| Socioeconomic Conditions | Age | 1,03 | 0,99-1,08 | 0,152 | 1,06 | 1,02-1,10 | 0,002 | |
| Gender (ref.: Man) | Women | 1,89 | 0,57-6,27 | 0,296 | 0,65 | 0,26-1,58 | 0,347 | |
| Schooling (ref.: < 3 years) | 4-7 years | 0,91 | 0,32-2,56 | 0,859 | 0,29 | 0,11-0,73 | 0,009 | |
| ≥ 8 years | 0,01 | 0,00--∞ | 0,989 | 0,15 | 0,02-0,81 | 0,028 | ||
| 1-2 salary | 0,51 | 0,07-3,97 | 0,526 | 0,40 | 0,08-1,86 | 0,247 | ||
| Income (ref.: < 1 salary) | >2 salary | 0,04 | 0,00-0,80 | 0,035 | 0,25 | 0,04-1,46 | 0,126 | |
| General Health | Alcoholic (ref.: no) | Yes | 0,69 | 0,20-2,32 | 0,55 | 0,54 | 0,20-1,48 | 0,238 |
| Multimorbidity (ref.: no) | Yes | 2,03 | 0,83-6,34 | 0,160 | 2,30 | 0,83-6,34 | 0,160 | |
| Oral Care | Use prosthesis(ref.: no) | Yes | 4,15 | 0,94-18,29 | 0,060 | 63,97 | 20,22-202,22 | <0,001 |
| Periodontal pocket (ref.: no) | Yes | 1,63 | 0,39-6,84 | 0,502 | 0,17 | 0,07-0,43 | <0,001 | |

| Variable | With functional dentition but anterior loss | No Functional Dentition | |||||||
| OR | IC95% | p | OR | IC95% | p- | ||||
| Oral changes after cancer treatment | Flavor change (ref.: no) | Yes | 0,31 | 0,10-0,90 | 0,032 | 0,62 | 0,26-1,45 | 0,276 | |
| Dental care | Brushing (ref.: no) | Yes | 0,50 | 0,18-1,39 | 0,186 | 0,22 | 0,09-0,53 | 0,001 | |
| Last consult (ref.: < 1 no) | ≥ 1 year | 1,42 | 0,48-4,17 | 0,519 | 1,41 | 0,59-3,34 | 0,427 | ||
Source: Author
IV. DISCUSSION
As far as we know, this is the first study to evaluate tooth loss and associated factors according to its number and location among cancer patients. There was found a high prevalence of tooth loss and approximately two thirds of the participants suffer from the absence of functional dentition. Among those who have at least twenty teeth, the losses of previous teeth are significant. Lower income and lack of taste alteration were associated with anterior losses, while the absence of functional dentition was higher among older and less educated individuals, those who use prosthesis, those who do not have periodontal pockets, and those who brush their teeth less than 3 times a day.
Regarding the number of teeth lost, two thirds of the participants did not have functional dentition. A study on tooth loss observed that among adults, had a maximum of 20 teeth[^17]. In the findings of Batista et al.[^2], of the evaluated lost 12 teeth or more. Yan et al[^26] observed that of patients reported having more than 10 missing teeth. It is pointed that these comparisons should be analyzed with caution, since the populations evaluated may differ in age and other characteristics that may directly influence the prevalence of tooth loss.
Even with considerable advances in recent decades in the dental area and in health services, Brazil is still a country with a high prevalence of tooth loss and oral health is not attributed due care[27]. The search for dental care in the recent past seems to be associated with the economic situation, in a directly proportional way[28]. With the inclusion of oral health in the Family Health Strategy in 2000 and the Specialty Centers in 2004, it is assumed that younger populations have benefited from the expansion of these services and they have changed from a mutilating and excluding health system to one that focused directly on the individual and on health promotion in an integral and general way[29], contributing to the reduction of tooth loss. Possibly, such actions along with improvements in socioeconomic conditions, especially in education and the health system, such as systemic and topical fluoridation and the widespread use of fluoridated toothpastes[^12], contributed to a reduction in the prevalence of dental caries, the main cause of tooth loss in Brazil2,10.
It is necessary to consider that not only the number, but the position of the missing teeth plays an important role in the determinants and consequences of tooth loss. The posterior teeth may be the most neglected mainly because they are located in non-aesthetic areas, making it difficult to perceive the need for treatment[^30]. The posterior teeth, however, have great importance in occlusion, chewing, phonation and have pits and fissures, considered as the first risk zone for caries in permanent dentition. Other studies have found similar results among individuals who have lost up to 12 teeth, including anterior teeth, and who therefore still have posterior teeth, are associated with a greater presence of caries and periodontal disease17,31. On the other hand, the anterior teeth exert influence on the appearance of the individual and assume a primordial role in personal and professional relationships. As the importance of facial aesthetics increased, the teeth began to gain relevance as aesthetic components of the smile, which results in an extensive search for treatments and care for the anterior region of the dental arch. While absent posterior teeth generate more noticeable impacts on function, the lack of anterior teeth promotes broader impacts on patients, affecting them not only in terms of pain and functional disabilities, but also in psychosocial dimensions[^32].
Lower income and lower schooling were associated with anterior losses and absence of functional dentition, respectively. These data corroborate the literature[2,17,33]. Individuals with lower incomes live in places with less access to dental treatments and lower water fluoridation coverage and have deleterious health habits such as smoking, ingesting more sugar and brushing their teeth less regularly . The economic situation and the education of individuals seem to be directly associated with the search for dental care . Schooling can be understood in its context as a parameter that contains the cultural, intellectual and educational background of the individual, which jointly will be responsible for determining life habits and attitudes, including those related to health and self-care . Understanding how the literature points out the relationship between oral health conditions and schooling is worrisome, since it can be noted that the most socioeconomically vulnerable population is also the most disadvantaged in terms of perception of health care. In addition, having less access to goods and services directly contributes to maintaining precariousness regarding self-care, general health and oral health aspects .
Bordin et al. (2017) concluded that the low frequency of tooth brushing was associated with fewer years of schooling, poor self-perceived oral health, tooth loss and smoking , which corroborates a study conducted in Turkey . Brushing teeth is a daily means of maintaining oral health and the lower frequency of brushing can contribute to the increased prevalence of periodontal disease and dental caries . Patients with better self-assessment of oral health regularly attend dental services, brush their teeth more frequently and consequently develop less oral problems .
The change of food flavor was more prevalent among patients with less tooth loss (those with functional dentition without anterior losses). This may reflect the level of self-perception, the interest and concern for oral health of those who have a satisfactory oral health condition. Among these patients, in addition to the number of teeth meeting functional demands, aesthetics also seems to meet expectations due to the absence of anterior losses. Some studies show that the perception of oral problems is higher precisely among those who have more access to dental services and, possibly, better oral health, which contributes to the awareness of its importance in these groups[^35].
The absence of periodontal pockets and the use of dental prosthesis were associated with the absence of functional dentition. Without the presence of the dental element, it is not possible to verify the periodontal pocket because, according to the adopted criteria, at least two functioning teeth are necessary to evaluate each sextant . This inference also occurs for dental prostheses. The more extensive the tooth loss, the greater the need and use of prostheses .
It is emphasized that for cancer patients oral problems may represent a secondary concern in the face of a life-threatening disease, which can alter all perceptions and influences regarding oral health and the patient's life . Adding this fact to the main findings of this study, it is pointed out the need for closer attention to the cancer public and its relationship with oral health. Most importantly, the need to encourage the search for dental treatment as a practice of self-care , highlighting the improvement in the clinical status of these patients . This is a priority demand, considering that only one third (33.3%) of the interviewed individuals reported having sought dental care in the last year.
Future studies should investigate the causes of the observed inequalities, in order to base and sustain intervention proposals to change this scenario. The strengths of this study are the use of instruments validated under international standards and widely used[22], which facilitates the comparability of its results with other studies. In addition, it seems that this is the first study to evaluate tooth loss and associated factors according to the number and location of the lost teeth among cancer patients. The limitation of the study is the means of randomization in obtaining the sample, since only the interested individuals sought participation in the study, and its cross-sectional design, which does not allow time inferences. However, it is important to point out the obstacles to obtain the sample with the population studied, given the difficulties generated by the patients' own health status, as well as issues related to the duration and periodicity of oncological therapies.
V. CONCLUSION
It was concluded that tooth loss has a relevant impact on cancer patients and, among the individuals with the highest number of teeth, the losses of previous teeth were significant. In addition, socioeconomic and oral health conditions were more strongly associated with the absence of functional dentition than anterior losses. These findings point to the need for dental care both in the prevention of tooth loss and in the attention to its resulting sequelae and limitations among cancer patients.



