



I. INTRODUCTION
The vast dissemination of smartphones and wearable devices has facilitated consumers to check, record and convey information about their physical pursuits, such as heart rate, temperature, calories incinerated and time elapsed while they were active physically (Talukder, Chiong, Bao, Malik, & Systems, 2018). A topic of global discussion is now centered on the impetuous inundation of technology and the continuous increase in the number of elderly people worldwide (Sharit & Czaja, 2017). According to data from World Population Prospects: the 2019 Revision, by 2050, one in six people in the world will be over age 65 (16%), up from one in 11 in 2019 (9%)
(United Nations, 2021). For instance, world's total elderly population aged 60 and above years is expected to rise by from 1 billion in 2019 to 2.1 billion in 2050 (Keating, 2022)(United Nations, 2021), where in Bangladesh, the number of older people is projected to stand at 36 million in 2050, with an annual growth of of the nation's total population (Help Age International, 2019), which means that one in every five Bangladeshi will be an older adult. Moreover, of world's total senior citizen will reside in Bangladesh along with other four Asian countries, namely, China, India, Indonesia and Pakistan together by 2025 (Chaklader, Haque, & Kabir, 2003). As the number of older adults in the country increases, so does the amount of non-communicable chronic diseases like heart attacks (Powell, Thompson, Caspersen, & Kendrick, 1987; Waxman, 2004), hypertension (Waxman, 2004), stroke (Wendel-Vos et al., 2004), diabetes (Sigal, Kenny, Wasserman, & Castaneda-Sceppa, 2004; Waxman, 2004), certain cancer (Slattery et al., 2003; Waxman, 2004) and obesity (Hill & Wyatt, 2005; Waxman, 2004), but people of all age-group can augment the quality of life by engaging themselves in physical activity. The World Health Organization (World Health Organization, 2010) has echoed that every adult should put their endeavor in moderate-level outdoor activities at least 150 min per week to ameliorate the physical and mental health as well as control the prevalence of chronic diseases. Since one third adults reside in Bangladesh exhibits physical in-activeness (Moniruzzaman et al., 2016), there is a need for a continuous effort to motivate them for engaging in physical exercise by the help of technologies, which can assist elderly people to change their behavior (Polap, Winnicka, Serwata, Ksesik, & Wozniak, 2018) though the rate of technology adoption by Bangladeshi is very poor (Barua & Barua, 2021; Barua et al., 2018; Sagib & Zapan; 2014). For example, wearable fitness trackers (WFT) are seen as a promising tool for individuals to take responsibility of one's own life and assist to self-monitor and self-regulate their fitness goals (Mercer et al., 2016). To achieve this, WFTs are designed to continuous keep tracking of physical activities such as steps walked, miles pedaled or traveled, number of calories intake or consumed, body temperature, heartbeat rate measurement, level of blood sugar, perspiration, sleeping pattern, floors climbed and sweat rate (Epstein, Jacobson, Bales, McDonald, & Munson, 2015; Shih, Han, Poole, Rosson, & Carroll, 2015) to provide users for getting easy access to their health-related information at any time and at any place (Akter, D'Ambra, & Ray, 2010). In current years WFT sales have risen and moreover, are going to be increased continuously by annually by 2023 (Prescient & Strategic Intelligence, 2018). The readily available WFTs not only keep tracking and monitoring physical activity but that also motivate or remind their users to do more—e.g., walked at least 250 steps per hour—are one way to promote healthy habits among health-conscious individuals (Lidynia, Brauner & Ziefle, 2017). Conversely, younger adults or generation Y who were born between the early 1980s and early 2000s (Horovitz, 2012), consists of about of the total population of Bangladesh (Statistics, 1991), accustomed to sedentary lifestyle like reading books or magazines, spending time in gossiping with friends and family or watching television, entertaining oneself by engaging in video games, or spending time in mobile phone/computer for significant time of the day instead of practicing sufficient physical activities like walking, playing, which is injurious to health and major contributor of many curable causes of mortality (WHO). Kruk (2009), clearly mentioned some adverse effects of the physical inactivity and the consequential health problems on countries. As a result, individuals either show their absenteeism in the workplace or they cannot exhibit their optimum performance due to illness; and a substantial number of resources have to expend for ensuring better treatment of these people that could be better used otherwise. Since younger adults in Bangladesh, similar to other developed nations, have no techno phobia as compared to other group of the marketplace (Sinkovics, Stöttinger, Schlegelmilch, & Ram, 2002), the mobility of a WFT, a big part of the internet of things (Sun, Ji, Wang, & Liu, 2016), has presented a ubiquitous stage for communication and personal fitness (Vooris, Blaszka, & Purrington, 2019). Rather than considered as 'technology', many younger adults also perceive WFT as 'fashion' or 'fashionology' (Hein & Rauschnabel, 2016). WFT could also move beyond the traditional devices that typically monitor health parameters in performance and hence can potentially obsolete these technologies in forthcoming healthcare system.
Whilst the efficacy of WFT is promising in this digital age (Butryn, Arigo, Raggio, Colasanti, & Forman, 2016; Mercer et al., 2016; Strath et al., 2011), their adoption has not met the expectations like other technological innovations, e. g., smartphones and tablets (Chau et al., 2019). This is because there has been relatively little research on the influence of age on fitness devices (Ehmen et al., 2012), although researchers on psychology have brought forward the role of age differences on technology adoption over the last few decades (Girard, 1993; Mc Carty & Shrum, 1993; Minton & Schneider, 1985). Additionally, WFTs are still in the early stage of commercialization, not much literature has been found on WFT in the context of Bangladesh. Therefore, this study seeks to investigate the intention of Bangladeshi to use WFTs and to comprehend the role of factors that affect this. To do this, this study could potentially present a starting point for the eventual successful introduction and implementation of the technology to address the issue of low physical activity levels among the Bangladeshi population. The results from this research may form part of the basis on which WFTs can be successfully implemented in Bangladesh to facilitate increased levels of physical activity among the population. Additionally, this research may contribute to the gap in knowledge that exists in regard to the adoption of wearable fitness trackers and the non-technical factors that affect it, as well as the gap that exists in literature about wearable fitness trackers and technology adoption in developing countries such as Bangladesh.
II. LITERATURE REVIEW AND RESEARCH MODEL
Several models have been used for measuring innovative technology adoption. Models such as the Theory-of-Reasoned-Action (TRA) (Fishbein & Ajzen, 1975), Technology-Acceptance-Model (TAM) (Davis, 1989), TAM2 (Davis, Bagozzi & Warshaw, 1989), TAM3 (Venkatesh et al. 2008), the Theory-of-Planned-Behavior (TPB) (Ajzen, 1991), the Unified-Theory-of-Acceptance-and-Use-of-Technology (UTAUT) (Venkatesh et al., 2003), UTAUT2 (Venkatesh, Thong & Xu, 2012), the Combined-TAM-and-TPB (C-TAMTPB) (Taylor & Todd, 1995), the Innovation-Diffusion-Theory (IDT) (Rogers, 1995) are employed to study the acceptance and/or use of technology. However, the research domain of technology acceptance has been ruled by the TAM and UTAUT, which are extensively used for inspecting IS adoption intention (Rahia et al., 2018). On the other hand, both of them were developed for measuring technology adoption from the organizational perspective (Venkatesh et al., 2012). Further, the explanatory power of the endogenous variables of those two models is low compared to the model UTAUT2, which was developed to measure individual consumer acceptance of technology. For instance, UTAUT model depict of the variance in BI and of the variance in use behavior (Venkatesh et al., 2012). Further, the UTAUT has four predicting variables (performance expectancy, effort expectancy, social influence, and facilitating conditions) whereas UTAUT2 is extended with three additional predicting constructs (habit, hedonic motivation, and price value). In addition, the explanatory power of UTAUT2 is better than the UTAUT (Venkatesh et al., 2012). The variance explained in BI and UB is and respectively in the UTAUT2, considered as substantial (Venkatesh et al., 2012).
However, previous research for investigating WFT adoption and use in the different contexts of the world used UTAUT2. For instance, Owen, Archibald, & Wickramanayake (2019) studied WFT adoption using UTAUT2 in Jamaica. Talukder et al. (2019) also used UTAUT2 in the Chinese context for investigating the key predicting variables of WFT adoption and use. Owen et al., (2019) extended the UTAUT2 by integrating 'perceived privacy and security risk' in the model as external variables. Further, Talukder et al. (2019) also extended the UTAUT2 model incorporating 'compatibility' and 'innovativeness' in the model. Further, Sergueeva, Shaw, & Lee (2020) suggest that the UTAUT2 model should further develop by incorporating other antecedents.
Considering the previous studies as well as better predictability of UTAUT2 for individual acceptance and use of technology, the current study also employed the UTAUT2 model. In addition, the model is further extended by encompassing 'health consciousness' of consumer as an additional variable to predict the WFT adoption and use in Bangladesh. The reason for incorporating health consciousness in the model is that, according to Hong (2011), it can influence the health behavior. Further, Cho, Park, & Lee (2014), regarding health technology use, noted that there is a substantial rapport between health consciousness and behavioral intention.
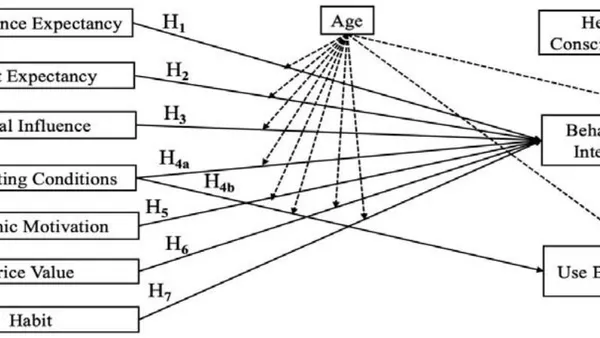
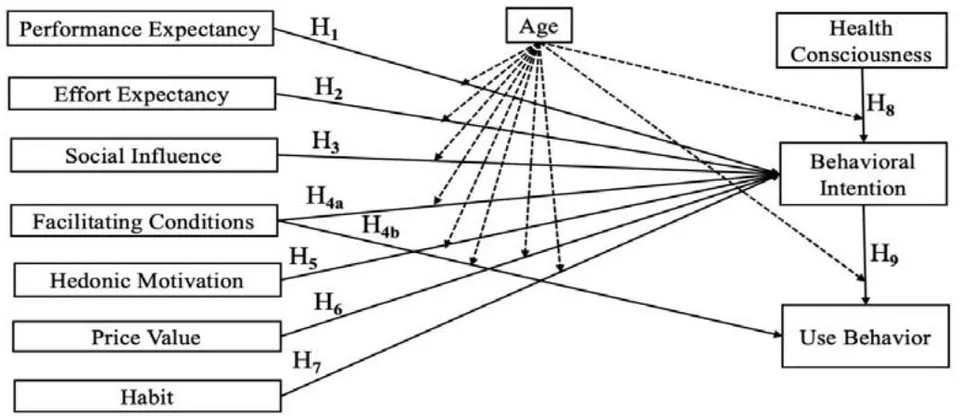
The current study also considered the role of age as moderating variable to investigate the differential effect of age on the relationship between exogenous and endogenous variables. The baseline UTAUT model and the extended UTAUT2 model also considered the age as moderating variable and found significant differences on the relationship between exogenous and endogenous variables. Researchers also stressed to investigate how age moderate the relationship among major accountable predictors of technology embracement (Venkatesh et al., 2003). Though age plays a critical role as moderator on the technology adoption and use (Venkatesh et al., 2003; Venkatesh et al., 2012), the variable did receive scant attention in the WFT adoption and usage in both developing and developed countries. However, the proposed model is presented in the Fig 1.
III. HYPOTHESES DEVELOPMENT
a) Performance Expectancy (PE)
PE, the premier construct of UTAUT2 model, is explicated by Venkatesh, Thong, and Xu (2012) as it refers to the magnitude to which one perceives that a certain job will be successfully carried out by using innovative technologies. In regard to WFTs, this predictor variable sets point to which an individual believes that the device has potential working power to track and monitor his/her physiological condition in a daily basis which finally do well his/her physical and mental health by reducing health related hazards. Reyes-Mercado and Technology (2018) reverberated that PE plays a pivotal role to augment the behavioral intention of users to adopt fitness wearable. Other studies reveal that older adult users residing in the community form certain specific expectations from technologies (Choudrie, Alfalah, & Spencer, 2017), which are not consistent with those expected by other segments of the marketplace. The above discussion wielded this research work to posit the following hypothesis:
: PE is positively associated with the elderly's intention to use WFT.
b) Effort Expectancy (EE)
Another cabbalistic construct of extended UTAUT model, EE point to the level of simplicity related with the use of a system (Venkatesh, Morris, Davis, & Davis, 2003). Technologies which are adroit at hassle avoidance and simple to use, users generally feel free to adapt these innovations swiftly to their own lives (Alalwan, Dwivedi, & Rana, 2017). In respect of WFTs, it is important to design these devices as unobtrusive technology which are easy to learn and get-at-able to operate for which consumers will hold firm determination to motivate users to adopt the technology (Dwivedi et al., 2016; Oliveira et al., 2014). In previous studies, it is explored that customers' chance of attaining comfort depends on the types of click and the age of customers (Venkatesh et al., 2003). Many of prior findings confirmed that perceived and real ease-of-use should take into consideration for making older adults highly inclined to adopt the technology (Cimperman et al., 2016). Therefore, we postulated the following hypothesis:
: EE is positively associated with the elderly's intention to adopt WFT.
c) Social Influence (SI)
Sl, another important constructs which have profound effect on consumer behavior to adopt a technology, is demarcated as the extent to which a person discerns that other people, who are placed by that person as reference group to which she/he belongs or hope to belong, envisage that a particular innovation should be adopted by him or her (Davis, 1989; Venkatesh et al, 2012). Although Venkatesh et al. (2003) did not notice a considerable effect on users' intention to adopt a technology in an organizational context in their study, Venkatesh et al. (2012) observe a remarkable influence of Sl. A number of extant literature revealed that consumers are likely to conform to others' expectations of their immediate reference groups for adopting new products (Venkatesh et al., 2003), i.e., WFTs, especially, when they have insignificant experience of the related innovation. Thus, based on these above findings, this study postulates:
: SI is positively associated with the elderly's intention to use WFT.
d) Facilitating Conditions (FC)
FC, a salient construct used in the research, is defined as the degree of perception to which an individual believes that an organizational and technical infrastructure remain to facilitate the use of an innovative system (Venkatesh et al., 2003). Extant literature opined that lacking sufficient FC, may create reluctance to actual use and thus significantly reduce the intention-to-use of a technology (Mahadeo, 2009). Because of age differences and inaptness with new innovations, the older adult users may demand more assistance than other age segments of the population to adopt and use of WFT (Gao et al., 2015). Likewise, we surmise that an augmentation in FC positively shaping the behavior of older adult users to adopt and use intention of WFT. Therefore, the stated argument urges to develop the following hypotheses:
: FC has a positive influence on the elderly's intention to use WFT (BI).
: FC is positively associated with elderly's actual use of WFT.
e) Hedonic Motivation (HM)
HM is related to fun or pleasure, an individual perceived from using a technology regardless of the performance consequences (Venkatesh et al., 2012). Theoretically, HM can be enunciated in terms of the intrinsic motivations that is driven by internal rewards from using new products, services, and applications; hence, such feelings of inherent satisfaction could drive the users to scrutinize the uniqueness of a new innovation (Venkatesh et al., 2012). For example, by wearing the sensors, users can continuously monitor the health related information such as sleep and calorie intake (Wei, 2014). These features assist WFTs to consider themselves more than just a fitness device and molding the intention of users to adopt and use it. Compared to other age groups of the population, young adults are tech savvy (Sultan et al., 2009) and are the early adopters of innovative technologies because of their eagerness for personal satisfaction or fulfillment (Gao et al., 2012). We, therefore, propose the following hypothesis:
: HM has a positive effect on behavioral intention to use WFT.
f) Price Value (PV)
PV, an important theoretical addition to the UTAUT2, is demarcated as settlement in consumers' thought process between the perceived values of the systems and the monetary cost incurred for using the technology (Venkatesh et al., 2012). Although WFTs are marketed to assist users to track and monitor the physical activities daily, some WFTs are deemed costly to purchase for low-income people (Gao et al., 2015). If users can obtain their health related information by using these devices, they can save both monetary and non-monetary costs by avoiding an unnecessary visit to the clinic or hospital. Since the inception of PV in the UTAUT2, some researchers (Alalwan et al., 2017; Arenas-Gaitan et al., 2015; Venkatesh et al., 2012) have demonstrated a positive relationship between PV and intention-to-use of a technology, while Oliveira et al. (2016) failed to report that PV has any significant impact on behavioral intention. Though these kinds of mixed findings are found in extant literature, this study supports the view that PV will significantly influence behavioral intention. So, this study has speculated the following hypothesis:
: PV positively influences behavioral intention to adopt WFT.
g) Habit (HT)
HT, an antecedent of behavioral intention to research technologies, is defined as the extent to which an individual exhibit instinctive behavior from learned behavior (Venkatesh et al., 2012). It is an acquired mode of behavior that is formed through frequently practice until it can be executed spontaneously and involuntarily (Huang and Yang, 2020). If an individual is accustomed to monitor physical condition by using WFTs, it will create an inside urgency to wear the devices automatically. Besides, it would be logically said that when an individual participate in health related activities, preliminary usage intentions will be rejuvenated, which positively drive to use frequently (Demiris et al., 2013). To agree with Alalwan (2020) and Barua and Barua (2021) HT is a regular tendency or practice by an individual to act automatically because of his or her holistic learning experience. Repeated usage behavior makes a habit, and, in turn, creates a positive inclination to adopt the technology. Amoroso and Lim (2017) found that customers who are delighted with their former experience of WFTs, show their constant eagerness to wear these devices incessantly. We, therefore, hypothesize that:
: HT has a positive effect on behavioral intention to use WFT.
h) Health Consciousness (HC)
HC is the extent to which an individual is concerned about ameliorating or maintaining his/her health (Lee & Lee, 2017). In addition, HC is an indication of the quality of people's life that drive him to undertake health actions (Kraft & Goodell, 1993). Prior studies on wearable technology devices have supported that there is a significant relationship between HC and BI (Lee & Lee, 2017; Wen et al., 2017). Patel, Asch (2015) proposed that wearable devices motivate users to increase physical activities, which in turn, improve healthy behavior. However, they admonish that one cannot improve his/her health by simply wearing these devices alone and to gain proper health, one have to engage himself/herself in positive health behavior practices. Hence, we deem that if an individual possess more health interest, she/he shows more intention-to-use the WFT. Based on these literatures, therefore, we posited the following hypothesis:
HC affects an individual's intention to adopt WFT.
i) Behavioral Intention (BI)
The relationship between the behavioral intention (BI) and actual use behavior (AUB) is well documented in many research fields and that indicates BI is the extent to which one intentionally determined to execute a given action (Islam et al., 2013). It has been experimentally proven that BI is positively related with the actual usage behavior of customers in different context (Taylor & Todd, 1995, Alam et al., 2020) BI was repeatedly used to measure as the attitudinal and behavioral loyalty. Furthermore, extant literature revealed that BI has significant impact on actual usage behavior (Goulão, 2014; Cimperman et al., 2016) Therefore, causal link between BI and the wearable use can be hypothesized as:
BI has a positive impact on the actual use of a WFT.
j) Age as Moderator
Technology acceptance and use decision is significantly influenced by individual differences (Arning & Ziefle, 2009). Age differences of the users plays a critical role in the technology adoption intention (Zhang et al., 2014). Technology adoption literature attracted the researchers to consider age as a moderator between endogenous and exogenous variables (Tavares and Oliveira, 2016). Morris & Venkatesh (2000) noted that technology usage decision is significantly differ for younger and older users. An empirical study by Alsswey and Al-Samarraie (2019) revealed that the relationship between ease of use and BI and usefulness and BI are significantly and positively influenced by age differences of the respondents (Alsswey and Al-Samarraie, 2019). Further, Zhu et al. (2018) noted that young people has shown strong association in adopting technology than middle-aged and older people. The above evidences helped the author to propose the following hypotheses:
: PE and WFT adoption intention is significantly moderated by age of the respondents.
: EE and WFT adoption intention is significantly moderated by age of the respondents.
: SI and WFT adoption intention is significantly moderated by age of the respondents.
: FC and WFT adoption intention is significantly moderated by age of the respondents.
: FC and WFT use behavior is significantly moderated by age of the respondents.
: HM and WFT adoption intention is significantly moderated by age of the respondents.
: PV and WFT adoption intention is significantly moderated by age of the respondents.
: HT and WFT adoption intention is significantly moderated by age of the respondents.
: HC and WFT adoption intention is significantly moderated by age of the respondents.
: BI and AUB adoption intention is significantly moderated by age of the respondents.
IV. RESEARCH METHODOLOGY
a) Measurement of Constructs
To test the proposed model, a survey was conducted introducing all the constructs' measurements statements of the conceptual model. The measurements items for all the constructs were adapted from the previously validated scale for ensuring the content validity. Considering the context of the study, some items were modified to fit the context. All the measurement items and their sources are listed in the appendix B.
b) Questionnaire Design, Sample Size and Data Collection
However, sample size was determined following the recommendation of MacCallum, Widaman, Zhang, and Hong (1999) who recommended that respondents to construct ratio is 20: 1. Our proposed model contains 10 constructs. Accordingly, a minimum sample size of 200 is suitable for this study. However, following the convenient sampling technique, the data were collected from 300 respondents for better explanatory precision of the model. Some responses were found problematic because of non-response bias, outliers problems etc. Finally, 288 responses were retained to test the relationship between variables and a set of hypotheses.
c) Data Analysis Technique
This study is an attempt to explore the key influential factors determining the use of WFT as well as to investigate the differential effects of age on the influential factors and dependent constructs. This study used Partial Least Squares-Structural Equation Modeling (PLS-SEM) to investigate the measurement and parameters of the constructs and the relationships between exogenous and endogenous variables. PLS-
SEM is widely used in information system research (Marcoulides and Saunders, 2006). An important advantage of PLS-SEM is that the small sample size could be operated in PLS-SEM. PLS-SEM is more appropriate for the analysis like determination of influential factors (Hair et al., 2016). As a PLS-SEM technique, this study employed SmartPLS 3.0 to analysis the data. Further, this study also employed SPSS 23 for determining the reliability and validity of the data.
V. RESULTS
a) Demographic Properties of the Respondents
Out of 288 respondents, were males and were females. respondents were less than the age of 40 and rest of them were 41 to 55 years. The majority of the respondents were service holders . respondents were engaged in business and were students. The majority of the respondents completed their Masters , where as respondents completed their Honors. Few of the respondents completed Higher-Secondary School Certificate and PhD . have been using WFT for less than a year, whereas respondents have 1 to 2 years of using WFT. respondents have 2 years of experience using WFT.
b) Common Method Bias (CMB)
Since the data is self-reported, CMB was inspected to circumvent the future risk to the outcome of the analysis. For examining CMB, primarily, this study checked the Harman's single factor test and found that variance is explained by a single factor from the overall variance where Podsak off & Organ (1986) suggested that less than indicates no presence of CMB problem. Correlation matrix was also checked and the correlation matrix indicates that there was no correlation greater than 0.90, a sign of absence of CMB. In addition, the CMB issues was also investigated based on Variance Inflation Factors (VIF) values (Table 1). All the VIF values range was 1.371 to 2.617 which are less than 3.3 (Kock, 2015). The statistical evidence indicates that CMB is not an issue for this study.
c) Measurement Model Validation
PLS algorithm was carried out in the SmartPLS3.0. One-tailed test with 0.05 significance level was employed. Based on the result, we checked the internal reliability, convergent validity, and discriminant validity for assessing the measurement model fit and validation (Hair et al., 2013). Internal reliability was ensured by assessing Cronbach's Alpha and Dijkstra-Henseler's rho . Cronbach's Alpha values for all constructs ranged from 0.752 to 0.894 (Table 1) and Henseler's rho values ranged from 0.786 to 0.901, indicates the reliability criteria successfully surpassed (Henseler et al., 2009).
| Constructs | Items | Loadings | Cronbach's Alpha | Rho_A | CR | AVE | VIF |
| Performance | PE1 | 0.859 | 0.881 | 0.883 | 0.918 | 0.737 | 2.210 |
| Expectancy | PE2 | 0.876 | 2.390 | ||||
| PE3 | 0.838 | 2.104 | |||||
| PE4 | 0.859 | 2.248 | |||||
| Effort | EE1 | 0.875 | 0.888 | 0.891 | 0.923 | 0.749 | 2.496 |
| Expectancy | EE2 | 0.859 | 2.165 | ||||
| EE3 | 0.881 | 2.550 | |||||
| EE4 | 0.847 | 2.203 | |||||
| Facilitating | FC1 | 0.804 | 0.831 | 0.832 | 0.888 | 0.664 | 1.720 |
| Condition | FC2 | 0.821 | 1.873 | ||||
| FC3 | 0.813 | 1.858 | |||||
| FC4 | 0.821 | 1.786 | |||||
| Social | SI1 | 0.839 | 0.853 | 0.865 | 0.900 | 0.693 | 1.958 |
| Influence | SI2 | 0.845 | 2.109 | ||||
| SI3 | 0.826 | 2.110 | |||||
| SI4 | 0.821 | 2.006 | |||||
| Price Value | PV1 | 0.905 | 0.809 | 0.894 | 0.884 | 0.717 | 1.785 |
| PV2 | 0.810 | 1.729 | |||||
| PV3 | 0.822 | 1.781 | |||||
| Hedonic | HM1 | 0.759 | 0.752 | 0.786 | 0.858 | 0.669 | 1.371 |
| Motivation | HM2 | 0.896 | 1.869 | ||||
| HM3 | 0.793 | 1.618 | |||||
| Habit | HT1 | 0.824 | 0.887 | 0.891 | 0.922 | 0.747 | 1.982 |
| HT2 | 0.859 | 2.281 | |||||
| HT3 | 0.889 | 2.611 | |||||
| HT4 | 0.884 | 2.614 | |||||
| Health | HC1 | 0.854 | 0.894 | 0.901 | 0.926 | 0.759 | 2.287 |
| Consciousness | HC2 | 0.879 | 2.617 | ||||
| HC3 | 0.866 | 2.472 | |||||
| HC4 | 0.885 | 2.440 | |||||
| Behavioral | BI1 | 0.883 | 0.858 | 0.859 | 0.913 | 0.778 | 2.103 |
| Intention | BI2 | 0.878 | 2.148 | ||||
| BI3 | 0.886 | 2.205 | |||||
| Actual Use | AU1 | 0.723 | 0.794 | 0.801 | 0.866 | 0.619 | 1.439 |
| Behavior | AU2 | 0.823 | 1.826 | ||||
| AU3 | 0.826 | 1.932 | |||||
| AU4 | 0.770 | 1.576 |
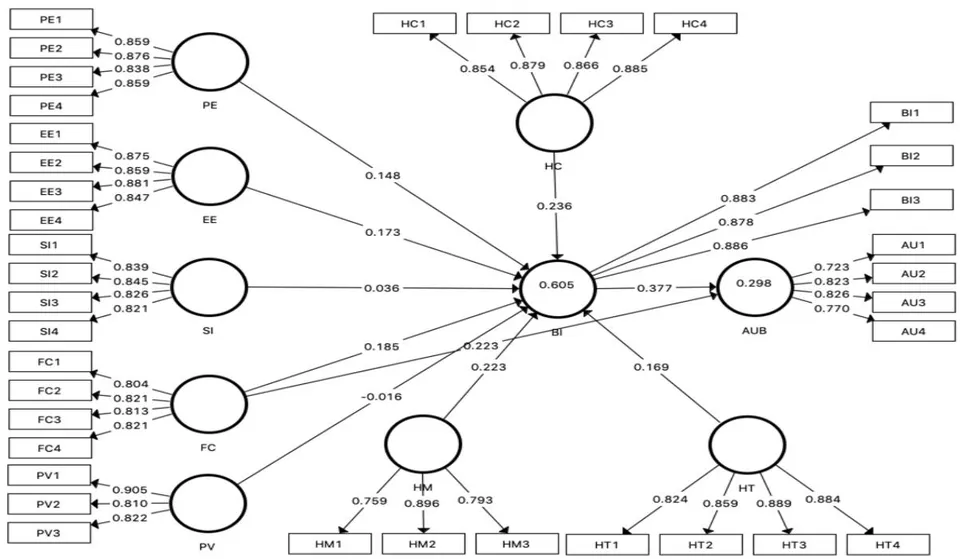
The convergent validity of the study was ensured by checking the criteria of item loadings, composite reliability (CR), and average variance extracted (AVE). Item loadings are found higher than 0.723 and composite reliability is greater than 0.884. further, AVE was found larger than the threshold limit 0.50 (Fornell and Larcker 1981). All the values of item loadings, CR, and AVE suggested that the model is convergently valid (Table 1 and Fig 2).
For discriminant validity, this study checked the Fornell-Larcker criterion and found that the square roots of AVEs are greater than the inter-correlation coefficients (Table 2). In addition, HTMT criteria was also checked and explored that all the HTMT ratios are much smaller than 0.90 (Table 3), indicates that model is discriminantly valid.
| AUB | BI | EE | FC | HC | HM | HT | PE | PV | SI | |
| AUB | 0.787 | |||||||||
| BI | 0.517 | 0.882 | ||||||||
| EE | 0.405 | 0.561 | 0.866 | |||||||
| FC | 0.460 | 0.628 | 0.513 | 0.815 | ||||||
| HC | 0.235 | 0.484 | 0.349 | 0.427 | 0.871 | |||||
| HM | 0.240 | 0.378 | 0.181 | 0.271 | -0.026 | 0.818 | ||||
| HT | 0.440 | 0.572 | 0.521 | 0.591 | 0.335 | 0.174 | 0.864 | |||
| PE | 0.476 | 0.607 | 0.539 | 0.590 | 0.386 | 0.307 | 0.534 | 0.858 | ||
| PV | 0.336 | 0.308 | 0.375 | 0.380 | 0.266 | 0.089 | 0.316 | 0.329 | 0.847 | |
| SI | 0.272 | 0.323 | 0.251 | 0.337 | 0.149 | 0.191 | 0.330 | 0.340 | 0.115 | 0.833 |
| AUB | BI | EE | FC | HC | HM | HT | PE | PV | SI | |
| AUB | ||||||||||
| BI | 0.623 | |||||||||
| EE | 0.48 | 0.64 | ||||||||
| FC | 0.57 | 0.74 | 0.60 | |||||||
| HC | 0.27 | 0.55 | 0.39 | 0.49 | ||||||
| HM | 0.31 | 0.46 | 0.22 | 0.34 | 0.09 | |||||
| HT | 0.52 | 0.65 | 0.59 | 0.69 | 0.38 | 0.21 | ||||
| PE | 0.57 | 0.70 | 0.61 | 0.69 | 0.43 | 0.38 | 0.60 | |||
| PV | 0.41 | 0.35 | 0.43 | 0.46 | 0.31 | 0.10 | 0.38 | 0.37 | ||
| SI | 0.33 | 0.37 | 0.29 | 0.40 | 0.17 | 0.24 | 0.37 | 0.38 | 0.14 |
VI. STRUCTURAL MODEL
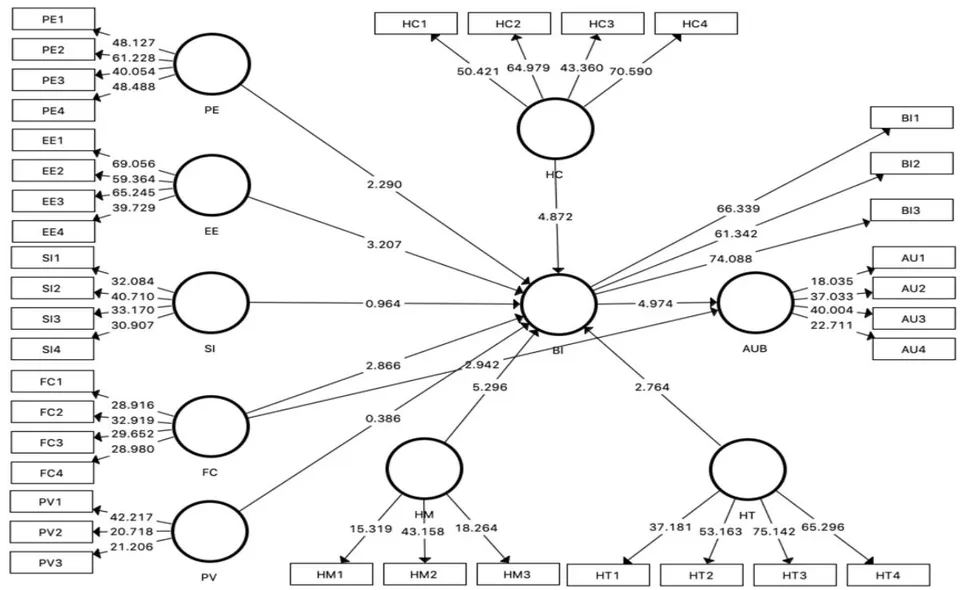
After surpassing the satisfactory requirements for measurement model, this study evaluated the structural model with 5000 resampling bootstrapping technique. Chin (1998) noted that the value of R2 of dependent construct can be used as the predictive power of the model. Falk and Miller (1992) noted that more than of variance explained by an endogenous construct indicates that a model is satisfactory and substantial. This study revealed that the R2 value for BI is and AUB is , indicates the model is suitable.
On the other hand, the result of hypotheses testing suggests that the SI (H3) and PV (H6) were not significant considering the significant level at . All other hypotheses i.e., eight out of ten hypotheses were revealed significant (Table 4 and Fig 3).
| Hypotheses | Relationships | Std Beta | Std Error | T-value | P Values | Comments |
| H1 | PE -> BI | 0.149 | 0.065 | 2.290 | 0.022 | Supported |
| H2 | EE -> BI | 0.168 | 0.054 | 3.207 | 0.001 | Supported |
| H3 | SI -> BI | 0.036 | 0.037 | 0.964 | 0.335 | Not Supported |
| H4a | FC -> BI | 0.183 | 0.064 | 2.866 | 0.004 | Supported |
| H4b | FC -> AUB | 0.226 | 0.076 | 2.942 | 0.003 | Supported |
| H5 | HM -> BI | 0.224 | 0.042 | 5.296 | 0.000 | Supported |
| H6 | PV -> BI | -0.010 | 0.042 | 0.386 | 0.700 | Not Supported |
| H7 | HT -> BI | 0.169 | 0.061 | 2.764 | 0.006 | Supported |
| H8 | HC -> BI | 0.236 | 0.048 | 4.872 | 0.000 | Supported |
| H9 | BI -> AUB | 0.379 | 0.076 | 4.974 | 0.000 | Supported |
a) Moderating Effect of Age
The moderating effect of age was tested by employing PLS- multigroup analysis (PLS-MGA). The respondents were divided into two groups namely, young (age less than 40) and elderly (age higher than 40) for operating PLS-MGA. As stated by Sarstedt et al.
(2011), PLS-MGA is the very conservative technique for assessing significant variations in multi-group. Significant variance in the two groups were tested and identified that the relationships between EE and BI, HT and BI, and HC and BI were significantly different for two groups as presented in the (Table 5).
| Parametric Test | ||||||||
| Young | Elderly | Young VS Elderly | ||||||
| Hypotheses | Relationships | Path coefficient | T-values | Path coefficient | T-values | T-values | P-values | Comments |
| H10a | PE -> BI | 0.067 | 1.021 | 0.209 | 2.209 | 1.256 | 0.210 | Rejected |
| H10b | EE -> BI | -0.011 | 0.215 | 0.267 | 2.833 | 2.568 | 0.011 | Accepted |
| H10c | SI -> BI | -0.023 | 0.488 | 0.111 | 2.054 | 1.888 | 0.060 | Rejected |
| H10d | FC -> BI | 0.145 | 1.763 | 0.073 | 0.743 | 0.572 | 0.568 | Rejected |
| H10e | FC -> AUB | 0.276 | 3.094 | 0.148 | 1.085 | 0.796 | 0.427 | Rejected |
| H10f | HM -> BI | 0.191 | 2.686 | 0.184 | 3.756 | 0.080 | 0.937 | Rejected |
| H10g | PV -> BI | 0.051 | 0.908 | -0.113 | 2.008 | 0.823 | 0.412 | Rejected |
| H10h | HT -> BI | 0.294 | 3.064 | 0.001 | 0.022 | 2.647 | 0.009 | Accepted |
| H10i | HC -> BI | 0.063 | 1.086 | 0.588 | 6.233 | 4.813 | 0.000 | Accepted |
| H10j | BI -> AUB | 0.316 | 3.236 | 0.433 | 3.526 | 0.751 | 0.453 | Rejected |
VII. DISCUSSION, IMPLICATIONS, AND LIMITATIONS
a) Discussions
This study applied the UTAUT2 model in Bangladesh context and attempted to extend it with the moderator of age. It examined age differences in perceptions of technology adoption and the relative importance of the factors affecting future intention to use WFT devices. Turning to the hypotheses, the results supported prior research indicating PE significantly influences an individual's acceptance of technology (Davis, 1989; Venkatesh, Morris, Davis, & Davis, 2003). The results indicate that WFT provides momentous benefits by allowing consumers to monitor, store and transmit information about their physiological and health related information, in turn, increase adoption and use among elderly people.
Along with PE, this study also aligned with literature suggesting EE is a direct determinant of usage behavior (Davis, 1989; Lee, Fiore, & Kim, 2006). For practitioners, perceiving EE as a vital construct in adoption and use is critical, especially during the diffusion process. The results suggest that lower effort in using WFT may result in higher propensity to adopt WFT. One of the key findings of the study does not support the role of SI on WFT continuance, describing the fact that factors that may lead to technology adoption may vary from culture to culture. Surprisingly, role of HM exhibit considerable relationship with WFT usage continuance. Consumers' inclination to use of wearables is motivated by the enjoyment they experience when using the technology. Today, WFTs are more than a simple self-tracking technology; they provide entertainment such as text message notifications and heath information in the form of colorful graphs, which consumers can easily read and share with their health care providers. This provides strong ground to belief that usage continuance is more intrinsically motivated rather than socially governed. In line with self-determination perspective, users of WFTs who have high health consciousness, they are more likely to continue the use of WFTs for continuously tracking their physiological condition. Contrarily, less motivated individuals may discourage to engage in physical activities to lead a healthy life and hence, discontinue the use of WFTs.
In addition, the results show that habit has significant positive influence on behavioral intention to adopt WFT. This indicates that continuously using WFT becomes the habit of users, as they need to wear 24/7 to monitor their daily activities. However, the results also show that price value is found to be not relevant to the context of WFT adoption which is consistent with the findings of other studies related to wearable devices (Talukder et al., 2019), as both have shown that price has no significant effect on intention to use technology. The most plausible reason for this that users are more conscious about attaining total perceived benefit by using WFT (Chan et al., 2012), in that case, the price issue do not play a major role for WFT adoption.
Facilitating conditions have a contributing effect on consumers' intention to use WFTs, which is consistent with other studies on adoption of wearable technology (Kim & Shin, 2015; Gao et al., 2015; Talukder et al., 2019; Kranthi & Ahmed, 2018; Reyes-Mercado, 2018). While a number of devices are marketed by addressing the target audience, there are few studies which have examined whether wearing the device strengthen a person's health consciousness (Coughlin & Stewart, 2016). The results of this study provide a preliminary realization about the potential benefit enjoyed from wearable devices regarding health consciousness. These findings recommend that people who wear a physical tracker are more health aware and active, as we considerably notice that wearing WFTs potentially increase the physical activity levels and create awareness among targeted population. Therefore, if the usage rate of WFT devices can be multiplied, users are likely to live a healthy lifestyle and be more active in engaging physical activities. This recommend that WFT devices have the potential to facilitate health behavior change.
b) Theoretical Contributions
This research has applied the UTAUT2 model to determine elderly behavioral intention to adopt WFT in the context of developing countries, e.g., Bangladesh. By ushering the moderating influence of age on the path-relationship among the constructs of UTAUT2 model along with an additional constructs, HC, however, this empirical research moves beyond the path-relationship what Venkatesh et al. (2012) have already suggested in their model. Prior studies have empirically investigated crucial factors from a technology perspective (Dehghani, Kim, Dangelico, & Informatics, 2018), but very few have examined WFT factors that affect consumers' intention to use WFTs in Bangladesh Context (Debnath, Kobra, Rawshan, Paramita, & Islam, 2018). The results explore that the proposed model has a good explanatory power in forecasting behavioral intention to use WFTs and this research provides a theoretical foundation for future emerging health information technology research from a behavioral perspective.
Age-specific differences played a moderating role in the relationship of EE and BI. For older adults, the EE played the main role in the adoption of WFT devices, whereas the EE had a lower explanatory power for younger adults. In addition, the causal relationship between HC and BI was more influential for older adults than for younger adults. This result provides a valuable insight into intention-to-use of WFT to monitor personal health among elderly people specially. One of the biggest concerns for practitioners is keeping consumers engaged with technology (Rejcek, 2016). In the past, consumers have discontinued the use of WFTs because the technology failed to meet their expectations regarding functionality and individual differences (Ledger & McCaffrey, 2014) (Ericsson, 2018; Ledger & McCaffrey, 2014). The results of this research provide some insights into WFTs to help market practitioners attract potential customers and retain existing customers. Many new improvements to WFTs will allow for the real-time consultation of personalized data by consumers and health care providers (Salah, Maclntosh, & Rajakulendran, 2014). This may ultimately increase engagement with the device and help elevate the level of consumer satisfaction about technology acceptance mostly among older people. In addition,
Marketers are also advised to make realistic claims about technology to create realistic consumer expectations and avoid future abandonment, thus engaging consumers to use this technology.
c) Practical Implications
However, regarding the moderating effects of user age, the findings show clearly, the relationship between HT and BI was stronger for participants of the younger age group. Since HT was a significant factor affecting a younger adult's intention to use WFTs, practitioners should put their endeavor on strengthening the habitual use of the product by proactively reinforcing the relationship with consumers. For example, companies might focus the personalized benefits and promote features that could assist in managing personal health. Customers and marketers, governments, insurance companies and the healthcare industry have great implications through the usage of WFT. As this research identified hedonic motivation, performance expectancy, and facilitating condition to be significant factors in behavioral intention to use WFTs, we recommend that to retain consumers, providers should design these technologies in a new-fashioned way for the end users to enhance enjoyment and engagement with WFTs. The recommendations can be used as new research model to foster the adoption intention of WFTs among users.
d) Limitations and Future Research Directions
Even though the present study provides some valuable insight with respect to intention-to-use and usage behavior of WFT in developing country context, this study is not out of some limitations that should be considered for the broader generalization and application of findings. The results assured that age has an important influence on technology usage in developing countries. However, two critical keystones should be envisaged in this context. The first is the taken sample of older adults is not representative for the population of the older age group. The older participants investigated here were comparably young and their academic qualification is quite satisfactory, therefore, future studies should examine older, and more representative samples. In doing so, older adults may retrieve optimum benefit from the utilization of WFT devices. Another shortcoming is that to overcome time and budget constraint, convenience sampling was used here as survey instrument for which the present study is suffered from some biasness because sample data failed to represent the entire population. In addition, only age differences as moderating variable is considered here, but other important individual differences e.g., the moderating effect of gender, experience of using technological devices, and educational level were not considered in this study. Therefore, since moderating effect reveal the deep insight (Barua et al., 2020; Barua,
2022), examining the effect of these moderating variables on the relationships among the endogenous and exogenous variables could provide some additional strong findings.
Based on these limitations, it is suggested that future studies should put their endeavor on identifying the preferences (e.g., color, language, layout and images) of elderly people from a cultural perspective and increase the adoption rate of these devices among them. In addition, future studies should focus on longitudinal surveys for better explanation of adoption and use behavior. Finally, the effect of other individual differences, such as gender, attitude and experience, should be taken into consideration to enhance the usage rate of WFTs among elderly people in future work.
Appendix A: Cross Loadings
| AUB | BI | EE | FC | HC | HM | HT | PE | PV | SI | |
| AU1 | 0.723 | 0.332 | 0.223 | 0.354 | 0.121 | 0.168 | 0.286 | 0.282 | 0.165 | 0.280 |
| AU2 | 0.823 | 0.461 | 0.356 | 0.390 | 0.223 | 0.214 | 0.361 | 0.436 | 0.257 | 0.178 |
| AU3 | 0.826 | 0.439 | 0.377 | 0.339 | 0.235 | 0.205 | 0.381 | 0.385 | 0.277 | 0.237 |
| AU4 | 0.770 | 0.385 | 0.306 | 0.364 | 0.148 | 0.164 | 0.350 | 0.381 | 0.352 | 0.171 |
| BI1 | 0.444 | 0.883 | 0.519 | 0.606 | 0.437 | 0.328 | 0.535 | 0.565 | 0.258 | 0.263 |
| BI2 | 0.448 | 0.878 | 0.471 | 0.525 | 0.394 | 0.367 | 0.506 | 0.519 | 0.233 | 0.280 |
| BI3 | 0.477 | 0.886 | 0.494 | 0.528 | 0.450 | 0.308 | 0.471 | 0.521 | 0.323 | 0.314 |
| EE1 | 0.371 | 0.479 | 0.875 | 0.441 | 0.314 | 0.158 | 0.439 | 0.457 | 0.310 | 0.227 |
| EE2 | 0.365 | 0.516 | 0.859 | 0.435 | 0.308 | 0.117 | 0.422 | 0.415 | 0.354 | 0.199 |
| EE3 | 0.310 | 0.497 | 0.881 | 0.431 | 0.297 | 0.167 | 0.473 | 0.527 | 0.313 | 0.219 |
| EE4 | 0.358 | 0.445 | 0.847 | 0.474 | 0.288 | 0.191 | 0.474 | 0.470 | 0.318 | 0.224 |
| FC1 | 0.376 | 0.513 | 0.440 | 0.804 | 0.366 | 0.215 | 0.485 | 0.476 | 0.344 | 0.264 |
| FC2 | 0.387 | 0.501 | 0.381 | 0.821 | 0.279 | 0.269 | 0.482 | 0.447 | 0.284 | 0.280 |
| FC3 | 0.333 | 0.505 | 0.440 | 0.813 | 0.320 | 0.222 | 0.502 | 0.565 | 0.317 | 0.311 |
| FC4 | 0.401 | 0.527 | 0.413 | 0.821 | 0.422 | 0.177 | 0.458 | 0.442 | 0.296 | 0.248 |
| HC1 | 0.226 | 0.394 | 0.319 | 0.402 | 0.854 | -0.053 | 0.297 | 0.331 | 0.209 | 0.161 |
| HC2 | 0.193 | 0.410 | 0.279 | 0.358 | 0.879 | -0.028 | 0.311 | 0.332 | 0.219 | 0.145 |
| HC3 | 0.156 | 0.391 | 0.311 | 0.354 | 0.866 | -0.048 | 0.280 | 0.320 | 0.276 | 0.114 |
| HC4 | 0.236 | 0.481 | 0.309 | 0.375 | 0.885 | 0.027 | 0.282 | 0.359 | 0.226 | 0.105 |
| HM1 | 0.134 | 0.281 | 0.061 | 0.152 | -0.119 | 0.759 | 0.116 | 0.200 | 0.050 | 0.158 |
| HM2 | 0.239 | 0.370 | 0.210 | 0.257 | 0.032 | 0.896 | 0.161 | 0.288 | 0.110 | 0.148 |
| HM3 | 0.208 | 0.263 | 0.157 | 0.251 | 0.006 | 0.793 | 0.148 | 0.262 | 0.048 | 0.170 |
| HT1 | 0.416 | 0.451 | 0.423 | 0.538 | 0.313 | 0.091 | 0.824 | 0.415 | 0.319 | 0.229 |
| HT2 | 0.368 | 0.485 | 0.428 | 0.477 | 0.258 | 0.167 | 0.859 | 0.481 | 0.292 | 0.253 |
| HT3 | 0.348 | 0.537 | 0.470 | 0.542 | 0.324 | 0.152 | 0.889 | 0.506 | 0.246 | 0.312 |
| HT4 | 0.397 | 0.499 | 0.478 | 0.487 | 0.263 | 0.186 | 0.884 | 0.439 | 0.243 | 0.340 |
| PE1 | 0.413 | 0.534 | 0.463 | 0.540 | 0.348 | 0.258 | 0.464 | 0.859 | 0.257 | 0.321 |
| PE2 | 0.395 | 0.553 | 0.470 | 0.478 | 0.346 | 0.259 | 0.457 | 0.876 | 0.297 | 0.286 |
| PE3 | 0.444 | 0.480 | 0.462 | 0.487 | 0.310 | 0.294 | 0.440 | 0.838 | 0.271 | 0.277 |
| PE4 | 0.386 | 0.513 | 0.455 | 0.523 | 0.318 | 0.248 | 0.472 | 0.859 | 0.303 | 0.283 |
| PV1 | 0.328 | 0.336 | 0.361 | 0.345 | 0.253 | 0.119 | 0.272 | 0.347 | 0.905 | 0.131 |
| PV2 | 0.227 | 0.201 | 0.279 | 0.260 | 0.212 | 0.049 | 0.214 | 0.184 | 0.810 | 0.008 |
| PV3 | 0.279 | 0.206 | 0.296 | 0.358 | 0.203 | 0.035 | 0.323 | 0.268 | 0.822 | 0.135 |
| SI1 | 0.219 | 0.305 | 0.232 | 0.365 | 0.170 | 0.150 | 0.296 | 0.324 | 0.139 | 0.839 |
| SI2 | 0.239 | 0.295 | 0.192 | 0.238 | 0.121 | 0.183 | 0.299 | 0.309 | 0.057 | 0.845 |
| SI3 | 0.249 | 0.228 | 0.203 | 0.225 | 0.065 | 0.155 | 0.231 | 0.236 | 0.058 | 0.826 |
| SI4 | 0.198 | 0.232 | 0.207 | 0.281 | 0.128 | 0.145 | 0.261 | 0.244 | 0.128 | 0.821 |
| Appendix B: List of Indicators | ||
| Item | Constructs and Statements | Sources |
| Performance Expectancy (EE) | Venkatesh et al. (2003); Venkatesh et al. (2012) | |
| PE1 | I find Wearable Fitness Technology is useful in my life. | |
| PE2 | Using Wearable Fitness Technology increases my chances of meeting my needs. | |
| PE3 | Using Wearable Fitness Technology helps me in managing my daily health fitness more quickly. | |
| PE4 | Using Wearable Fitness Technology service increases my capability to manage my health fitness. | |
| Effort Expectancy (EE) | Venkatesh et al. | |
| EE1 | Learning how to use Wearable Fitness Technology is easy for me. | (2003);Venkatesh et al.(2012) |
| EE2 | My interaction with Wearable Fitness Technology is clear and understandable. | |
| EE3 | I find Wearable Fitness Technology easy to use. | |
| EE4 | It is easy for me to become skillful at using Wearable Fitness Technology. | |
| Price Value | ||
| PV1 | Wearable Fitness Technologies are reasonably priced. | Venkatesh et al.(2012) |
| PV2 | Usually, Wearable Fitness Technologies are a good value for the money. | |
| PV3 | At the current price, Wearable Fitness Technologies provide a good value. | |
| Social Influence (SI) | Venkatesh et al.(2003);Venkatesh et al.(2012) | |
| SI1 | People who are important to me think that I should use Wearable Fitness Technology. | |
| SI2 | People who influence my behavior think that I should use Wearable Fitness Technology. | |
| SI3 | People whose opinions that I value prefer that I use Wearable Fitness Technology. | |
| SI4 | People in my society who use Wearable Fitness Technology are more prestigious than those who do not. | |
| Facilitating Condition (FC) | Venkatesh et al.(2003);Venkatesh et al.(2012) | |
| FC1 | I have the resources necessary to use Wearable Fitness Technology. | |
| FC2 | I have the knowledge necessary to use Wearable Fitness Technology. | |
| FC3 | Wearable Fitness Technology is compatible with other technologies I use. | |
| FC4 | I can get help from others when I have difficulties using Wearable Fitness Technology. | |
| Hedonic Motivation (HM) | ||
| HM1 | Using Wearable Fitness Technology is fun. | |
| HM2 | Using Wearable Fitness Technology is enjoyable. | Venkatesh et al.(2012) |
| HM3 | Using Wearable Fitness Technology is entertaining. | |
| Habit (HT) | ||
| HT1 | The use of Wearable Fitness Technology has become a habit for me. | Venkatesh et al.(2012) |
| HT2 | I am addicted to using Wearable Fitness Technology. | |
| HT3 | Using Wearable Fitness Technology would be a regular activity for me. | |
| HT4 | Using Wearable Fitness Technology has become natural to me. | |
| Health Consciousness (HC) | ||
| HC1 | I think it is important to know well how to stay healthy | Chen (2011) |
| HC2 | My health is so valuable to me that I am prepared to sacrifice many things for it | |
| HC3 | I have the impression that I sacrifice a lot for my health | |
| HC4 | I consider myself very health conscious | |
| Behavioral Intention (BI) | Venkatesh et al.(2012); Taylor and Todd (1995) | |
| BI1 | I intend to continue using Wearable Fitness Technology in the future. | |
| BI2 | I will always try to use Wearable Fitness Technology in my daily life. | |
| BI3 | I plan to continue to use Wearable Fitness Technology frequently. | |
| Actual Use Behavior (AUB) | ||
| AUB1 | Wearable Fitness Technology provide me a pleasant experience. | Venkatesh et al.(2012); Taylor and Todd (1995) |
| AUB2 | I really use Wearable Fitness Technology to keep my health fit. | |
| AUB3 | I spend a lot of time on Wearable Fitness Technology. | |
| AUB4 | I use Wearable Fitness Technology on regular basis. | |



