Testicular seminoma commonly occurs in young men aged between 15 and 45 years old. Those with testicular cancer may present with a lump or swelling in the testicle. If treated and managed early, patients can expect a greater than 90% success rate. However, advanced stages of testicular seminoma can lead to eventual metastasis. We present a 45-year-old male patient with a prior history of testicular seminoma who was admitted to the emergency department with abdominal distension and mild abdominal pain. The CT identified a rather sizable abdominal mass and the biopsy report confirmed metastatic testicular seminoma. This patient is currently on active chemotherapy with bleomycin, cisplatin, and etoposide.
## I. INTRODUCTION
Testicular cancer represents $1\%$ of male tumors and $5\%$ of urological cancers (1) and predominantly affects young males between the ages of 15 and 45 years old (2). With early diagnosis and intervention, the prognosis is promising with greater than $90\%$ cure rate and $95\%$ five-year survival rate (1). There is a multitude of factors that can cause testicular cancer including cryptorchidism (2-4-fold increased risk) (3), family history of testicular cancer (6-10% fold increased risk) (4), prior history of testicular cancer (1), sexually transmitted infections (5), testicular trauma (6), and potentially elevated maternal estrogen levels (7). There may be no prominent symptomology for patients with testicular cancer (8). However, some patients may experience painless swelling and other less common symptoms such as back pain, enlargement or tenderness of breast tissue and pain in the lower abdomen (8).
### Case Report
A 45-year-old man with prior medical history of testicular cancer and left orchiectomy in 2021 was admitted to the emergency room with mild abdominal pain, distention, and vomiting. Our patient reported missed outpatient attendance following their orchidectomy in 2021. He had no known testicular cancer in his family history. Additionally, there is no medical history of cryptorchidism. On initial presentation, his heart rate was 130, blood pressure was 130/70, respiratory rate of 16, oxygen saturation was $98\%$ and he was afebrile. His tachycardia improved with fluid resuscitation. On physical examination, a large, distended abdomen and generalized abdominal tenderness was noted. His bowel sounds were present, and previous surgical scars healed well.
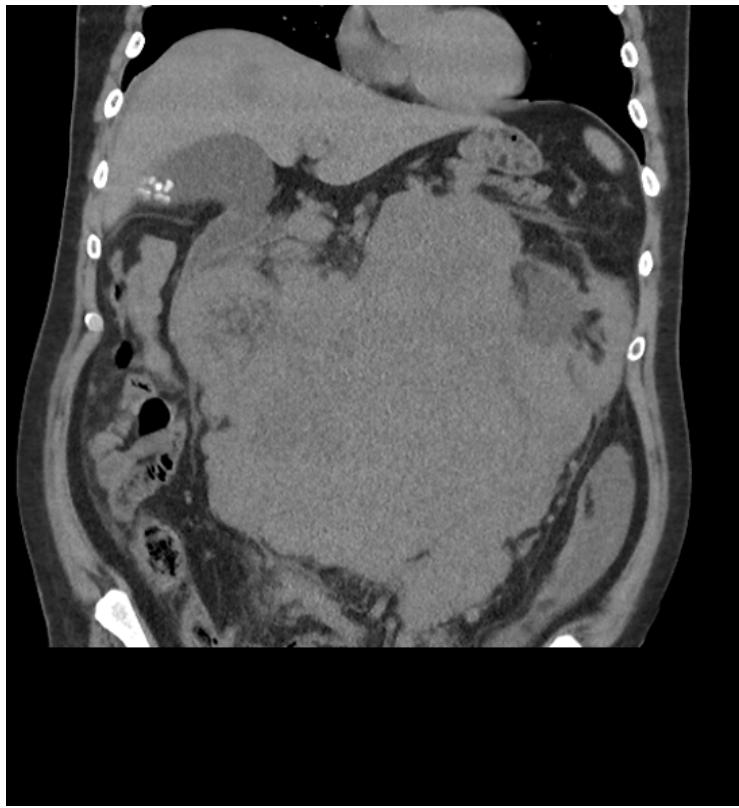
The abdominal and pelvic CT in Figure 1 and Figure 2 revealed a large undifferentiated mass localized throughout the abdomen and pelvis (transverse dimensions: $25.4 \times 22.8$ cm). The CT scan in Figure 1 also demonstrated left kidney displacement and encasement of the abdominal aorta, visceral branches, and inferior vena cava. There is also encasement of the small and large bowel loops in the upper abdomen and this mass extends into the central pelvis. The liver in Figure 2 also highlights one of the many multiple solid lesions spread throughout both hepatic lobes and is mainly right-sided. The largest solid lesions in segment 6 and 4A are respectively measuring up to $3.2$ cm and $2.9$ cm. Our patient proceeded to have further staging scans which did not reveal any metastatic depositions to the chest, head, and neck.
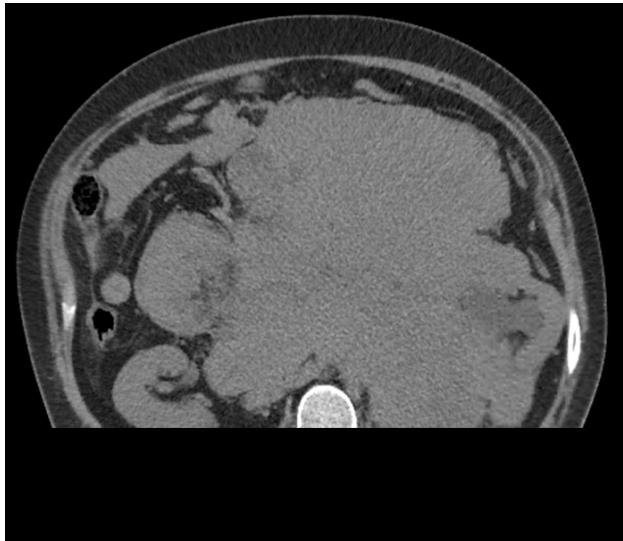 Figure 1: Axial slice of the abdomen noting large conglomerate mass located centrally with significant displacement of the left kidney and the small bowels. This mass measures up to $25.4 \times 22.8\mathrm{cm}$ in transverse directions
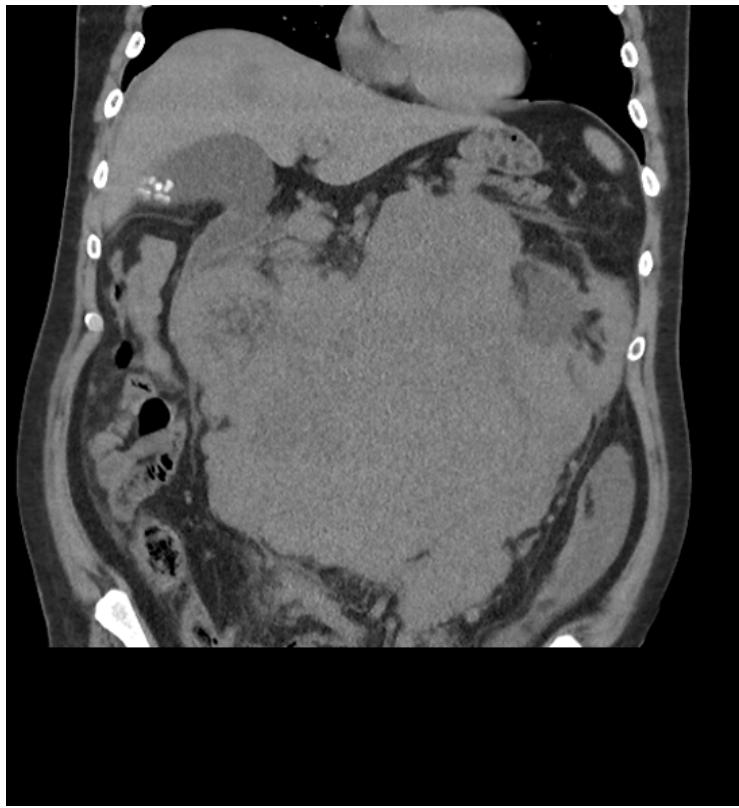 Figure 2: Coronal slice of the abdomen noting same mass with significant displacement of the bowels. A hypodense lesion can be visualised on the liver
Histopathology presented sheets of polygonal cells with substantial clear cytoplasm and vesicular nuclei, with dispersed lymphocyte-rich septa. Immunohistochemistry revealed that the tumor cells are positive for PLAP, OCT3/4 and CD117 and negative for SOX10. Hence, this histologic evaluation was deemed to be consistent with the diagnosis of metastatic seminoma for our patient.
The current oncologic diagnosis of this patient is stage IIc seminoma. The oncologic history is pure seminoma PT1bNx with left orchiectomy in 2021. The tumor markers for this admission are alpha-fetoprotein (AFP) at 4.4, Lactate dehydrogenase (LDH) at 1230, and beta-human chorionic gonadotropin $(\beta -hCG)$ at 38. He was admitted under the oncology team and started chemotherapy. He has been scheduled for 4 cycles of chemotherapy and is currently on bleomycin, etoposide, and platinum (BEP) therapy.
## II. DISCUSSION
This is a unique case of a patient presenting with abdominal distension. Abdominal distension is a common presentation to the emergency department and has a wide range of differentials (9). It is important to obtain a thorough medical history and physical examination of the patients before requesting an investigation. This patient had a left orchiectomy in 2021 and was noted to miss most of his follow-up appointments. It is important to consider imaging of these subset of patients with oncological history and has been more routinely performed in the emergency department in recent years.
Seminomas are germ cell tumors that account for up to $50\%$ of all testicular tumors (10). These tumors metastasize within the lymphatic system with the retroperitoneal lymph nodes being the most common sites (10). The risk factors for seminomas are cryptorchidism (3), family history of testicular cancer (4), prior history of testicular cancer (1) and testicular trauma (6). This patient has a prior history of testicular cancer. His AFP was within normal levels, which is consistent with seminoma. His LDH was 1230 which is 2.5-fold above the upper normal limit for LDH.
One third of seminoma patients present with metastatic disease (10). There are different chemotherapy medications and regimens currently in use to manage this condition. This patient is currently on treatment with BEP. BEP was studied in a randomized control trial in 1980 against cisplatin, vinblastine, and bleomycin (PVB) (11). This study had a total of 244 patients, with 121 patients treated with BEP compared to 123 in PVB. $74\%$ of patients with PVB became disease-free compared to $83\%$ with BEP therapy. Neuromuscular toxicity was significantly less in BEP than that of PVB, favoring BEP therapy.
The results from the International germ-cell cancer collaborative group (IGCCG) compared the current data to that of original data from the 1980s for metastatic seminoma (10). The progression free survival rate (PFS) has improved from 82 to $89\%$ with a $95\%$ confidence interval between 87 to $90\%$ with BEP therapy in favor of the current data. The 5-year overall survival rate in the modern series is $95\%$ to that of $86\%$ in the 1980s with confidence interval between 94 to $96\%$ in patients with a good prognosis. For intermediate prognosis, the overall survival has improved from $72\%$ to $88\%$ with $95\%$ confidence interval between $80 - 93\%$.
LDH has been recommended for assessment of the prognostic factor for seminoma cancer. Patients with good prognosis with LDH 2.5-fold above the normal limit had a 3-year progression free survival rate of $80\%$ and overall survival of $92\%$. Patients with lower LDH level are noted to have a progression free survival rate of $92\%$ and overall survival of $97\%$ (10). This patient will be classed poor prognosis given the abdominal metastasis with LDH levels 2.5-fold above the normal upper limit. His current estimated 2-year survival rate is $36\%$ with $95\%$ confidence interval between 12- $60\%$.
Most testicular cancers exist as a mass localized to the testicle and thereby presents as a painless testicular mass which can progress to a significant size. With early diagnosis and effective management, patients can expect to lead a good quality of life following treatment. However, this patient reported poor attendance in follow up consultations after their testicular cancer diagnosis and orchidectomy in 2021. This resulted in a significant palpable metastatic mass present in their abdominal region as the initial manifestation from testicular seminoma confirmed via CT scan and histological assessment. This patient is currently on bleomycin, etoposide, and platinum (BEP) therapy and is scheduled for four cycles of chemotherapy.
## III. CONCLUSION
Testicular feminoma is a common malignancy amongst young men between the ages of 15 and 45 years old (2). Most patients will not experience obvious symptoms. However, there may be a subset of patients experiencing less common symptomatology such as abdominal and back pain. Perhaps young men experiencing regular, painful bouts of abdominal pain should also be considered for testicular cancer especially if the patient has a history of testicular malignancy.
### ACKNOWLEDGEMENT
#### Funding Statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
#### Conflict of Interest
The authors declare no conflict of interest in preparing this article.
Generating HTML Viewer...
References
11 Cites in Article
S Gaddam,G Chesnut (2023). Testicle Cancer. Stat Pearls. Treasure Island.
Jee Park,Jongchan Kim,Ahmed Elghiaty,Won Ham (2018). Recent global trends in testicular cancer incidence and mortality.
L Ferguson,A Agoulnik (2013). Testicular cancer and cryptorchidism.
R Del Riscokollerud,E Ruud,H Haugnes,L Cannon-Albright,M Thoresen,P Nafstad (2019). Family history of cancer and risk of paediatric and Unusual Case of Large Conglomerate Mass in Abdomen Global Journal of Medical Research ( D ) XXIV Issue I Version I Year 2024 young adult's testicular cancer: A Norwegian cohort study.
Andrea Garolla,Amerigo Vitagliano,Francesco Muscianisi,Umberto Valente,Marco Ghezzi,Alessandra Andrisani,Guido Ambrosini,Carlo Foresta (2019). Role of Viral Infections in Testicular Cancer Etiology: Evidence From a Systematic Review and Meta-Analysis.
Brenda Haughey,Saxon Graham,John Brasure,Maria Zielezny,Gerald Sufrin,William Burnett (1989). THE EPIDEMIOLOGY OF TESTICULAR CANCER IN UPSTATE NEW YORK.
R Depue,M Pike,B Henderson (1983). Estrogen exposure during gestation and risk of testicular cancer.
(2025). Testicular Cancer: Types, Symptoms, Diagnosis, and Treatment.
Amir Mari,Fadi Abu Backer,Mahmud Mahamid,Hana Amara,Dan Carter,Doron Boltin,Ram Dickman (2019). Bloating and Abdominal Distension: Clinical Approach and Management.
Jörg Beyer,Laurence Collette,Nicolas Sauvé,Gedske Daugaard,Darren Feldman,Torgrim Tandstad,Alexey Tryakin,Olof Stahl,Enrique Gonzalez-Billalabeitia,Ugo De Giorgi,Stéphane Culine,Ronald De Wit,Aaron Hansen,Marko Bebek,Angelika Terbuch,Costantine Albany,Marcus Hentrich,Jourik Gietema,Helene Negaard,Robert Huddart,Anja Lorch,Fay Cafferty,Daniel Heng,Christopher Sweeney,Eric Winquist,Michal Chovanec,Christian Fankhauser,Daniel Stark,Peter Grimison,Andrea Necchi,Ben Tran,Axel Heidenreich,Jonathan Shamash,Cora Sternberg,David Vaughn,Ignacio Duran,Carsten Bokemeyer,Anna Patrikidou,Richard Cathomas,Samson Assele,Silke Gillessen (2021). Survival and New Prognosticators in Metastatic Seminoma: Results From the IGCCCG-Update Consortium.
Stephen Williams,Robert Birch,Lawrence Einhorn,Linda Irwin,F Greco,Patrick Loehrer (1987). Treatment of Disseminated Germ-Cell Tumors with Cisplatin, Bleomycin, and either Vinblastine or Etoposide.
No ethics committee approval was required for this article type.
Data Availability
Not applicable for this article.
How to Cite This Article
Sajanakan Sriselvakumar. 2026. \u201cUnusual Case of Large Conglomerate Mass in Abdomen\u201d. Global Journal of Medical Research - D: Radiology, Diagnostic GJMR-D Volume 24 (GJMR Volume 24 Issue D1).
Explore published articles in an immersive Augmented Reality environment. Our platform converts research papers into interactive 3D books, allowing readers to view and interact with content using AR and VR compatible devices.
Your published article is automatically converted into a realistic 3D book. Flip through pages and read research papers in a more engaging and interactive format.
Our website is actively being updated, and changes may occur frequently. Please clear your browser cache if needed. For feedback or error reporting, please email [email protected]
Thank you for connecting with us. We will respond to you shortly.